Gastroenterology and Hepatology Research
OPEN ACCESS | Volume 7 - Issue 1 - 2026
ISSN No: 2836-2888 | Journal DOI: 10.61148/2836-2888/GHR


Ramesh Satarkar 1*, Anuj Satarkar 2
1 Gastroenterology Center, 20, Tilaknagar, Near Savarkar chowk, Dargah road, Aurangabad.
2 Gastroenterology center aurangabad, 431005. Maharashtra, india
*Corresponding author: Beltagi M, Gastroenterology Center, 20, Tilaknagar, Near Savarkar chowk, Dargah road, Aurangabad.
Received date: May 06, 2021
Accepted date: May 10, 2021
Published date: May 17, 2021
Citation: Ramesh Satarkar and Anuj Satarkar. (2021) “Pill Esophagitis: Novel Therapeutic Approach to A Preventable Disease.”, J of Gastroenterology and Hepatology Research, 2(2); DOI: http;//doi.org/05.2021/2.1011.
Copyright: © 2021 Ramesh Satarkar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
Medication induced esophageal injury (Pill esophagitis) is an uncommon but important adverse effect of many medications. Patient factors like esophageal motility disorders, esophageal narrowing, taking medications with inadequate water or in lying down position predispose to `Pill esophagitis`. Doxycycline, NSAIDs, potassium chloride, Alendronate are common medications which are responsible for majority of the cases described. Most published literature is in the form of case reports or short case series. We report 17 patients of pill esophagitis from our center.
Introduction:
Medication induced esophageal injury is an uncommon but important and preventable adverse effect of some medications and formulations. Majority of the cases are caused by tetracycline, doxycycline, potassium chloride, non- steroidal anti- inflammatory drugs (NSAIDs), and alendronate sodium although the list is extensive [1,2,3]. The overall incidence of medication induced oesophageal injury has been estimated at 0.004% per year in United States of America, but ranges from 0.04% for alendronate sodium to as high as 20% for NSAIDs. Since women are more likely to be treated with high-risk medications, they are twice as likely as men to have medication induced esophageal injury [1,4].
In majority of the patients the factor responsible is taking the pills with inadequate water, or in lying down position or lying down immediately after taking the medication. Certain patient factors like esophageal dysmotility, luminal narrowing, predispose to this condition.
Material and methods:
We analyzed our hospital case records from 2005 to 2019 and found 17 patients of pill esophagitis at our center during this period. Patient demography, culprit medication, endoscopic findings and response to treatment were studied and are presented.
Results:
There were 40 patients of acute, benign, non-GERD, esophageal ulcers during this period. Of these 17 qualified for the diagnosis of pill esophagitis as they had definite history of exposure to medicines capable of causing pill esophagitis. There were 12 female and 5 male patients. Age ranged from 18 years to 47 years. Maximum (8) patients were in the age group 21-30 year (Table 1).
|
Age group |
Male |
Female |
Total |
|
11-20 |
1 |
2 |
3 |
|
21-30 |
3 |
5 |
8 |
|
31-40 |
1 |
4 |
5 |
|
41-50 |
0 |
1 |
1 |
|
Total |
5 |
12 |
17 |
Table 1: Age and sex distribution of patients.
Fifteen patients had Odynophagia while eleven had dysphagia. Mean duration of symptoms was 5 days with a range of 2 to 15 days. Three patients had retrosternal chest pain and three had backache. None had vomiting or hematemesis. 13 patients had definite history of consumption of Doxycycline capsules and 4 had history of NSAID consumption (2 Aceclofenac,2 Over the counter) prior to onset of symptoms. Majority patients gave history of consumption of tablets with inadequate water or in lying down position. None of the patients had prior history of esophageal motility disorder. The commonest indication of use of Doxycycline was pelvic inflammatory disease in female patients and dental treatment in male patients (Table 2).
|
|
Male |
Female |
Total |
|
Doxycycline |
4 |
9 |
13 |
|
NSAIDs |
1 |
3 |
4 |
|
Total |
5 |
12 |
17 |
Table 2: Culprit medication and its sex distribution.
In all the patients HSV IgM AB, CMV IgM Ab and HIV Ab were done to exclude competing etiology and were negative in all.
Esophago- gastroscopy was done in 14 patients and revealed single ulcers in 3 and multiple aphthous like ulcers in 11 patients. In all the patients, the ulcers were in mid-esophagus between 20 to 30 cm from incisors. Ulcers were superficial, variable in size and had flat edges (Figure 1).
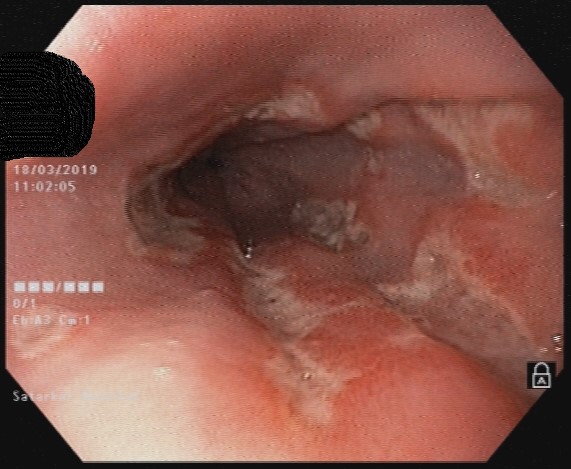
Figure 1: Endoscopic image of pill esophagitis.
Biopsy was done in 4 patients in whom additional pathology like viral infection or tuberculosis was suspected especially if history exceeded one week. It revealed acute esophagitis in one and nonspecific esophageal inflammation in three patients.
Culprit medication was stopped in all patients immediately. Patients were treated with a combination therapy of either Nifedepine or Hyoscine butyl bromide, local anesthetic agents (Xylocaine viscus or Oxetacaine) and liquid antacids. Twelve patients received Nifedepine tablets 10 mg twice a day, 30 min before food. Of these two patients received only Nifedepine while 10 received it along-with local anesthetic agent and liquid antacids. All these patients were normotensive before starting Nifedepine. On follow up none had hypotension. Five patients received Hyoscine butyl bromide 10 mg 6 hourly along-with liquid antacids and local anesthetic agents. Xylocaine Viscus was used as local anesthetic agent in 8 patients while Oxetacaine containing antacids in three patients. Six patients received alginate containing liquid antacids while two patients received sucralfate. Choice of medication was random.
Ten patients came for follow up. All of them made complete recovery within one week and became symptom free. No patient had any adverse event with treatment medication. Repeat endoscopy was not done in any patient. Seven patients were lost to follow up. Of these 6 patients were in Nifedepine group while one was in Hyoscine group.
Discussion:
Medication induced esophageal injury or Pill esophagitis is a rare but significant adverse event of certain medications. The incidence varies according to the medication. The published literature is scanty because the disease is unrecognized many times and under reported. However, it is important to report the cases as it can help in spreading awareness about this potentially preventable complication. List of responsible medications is extensive and over one hundred medications have been reported to be responsible for this problem [3]. Even homeopathic pill has been reported to cause pill esophagitis [5]. However, in today`s era common offending agents are Doxycycline, NSAIDs, Alendronate and potassium chloride. Our series also had all the cases distributed between Doxycycline and NSAIDs [1,2,3].
Women are twice more likely to be affected than men probably because they are more likely to consume the offending agents. We had similar experience with 12 out of 17 patients being women. Patients with esophageal motility disorders, esophageal stricture are more likely to be affected because of higher chances of the pill getting stuck. None of our patient had pre-existing esophageal structural or functional disease. Majority patients have normal esophageal structure and function and in them the factor responsible is taking the pill with inadequate water or taking pills in reclining position or to lie down immediately after taking the medication. The physical form of the delivery system of the medication, its chemical composition are also important factors. When 18 normal subjects swallowed gelatin capsules with water while upright, the capsules remained in the esophagus longer than 5 minutes in 11 subjects. Pills were even more likely to stick if swallowed without water or while supine. Tetracyclines, ascorbic acid, and ferrous sulfate all produce acidic solutions (pH < 3.0) when dissolved in 10 ml of water, suggesting that they may produce acid burns. Phenytoin sodium produces an alkaline solution and may produce an alkaline burn [6].
Odynophagia is hallmark of pill esophagitis. It is sudden onset with temporal relationship to the medication consumption. Pill esophagitis should be suspected whenever a patient presents with the sudden onset of odynophagia even when pills have been taken properly [3]. Fifteen out of our 17 patients had odynophagia. Eleven patients had dysphagia, three had chest pain and three had backache. None had vomiting or gastrointestinal bleeding. GI bleeding is an uncommon but significant symptom of NSAID induced mucosal ulcers and can be severe requiring transfusions or even life threatening. Kikendall noted that 22 of 154 NSAID-induced esophageal injuries were complicated by hemorrhage. In contrast, only 25 of 796 esophageal injuries induced by other medications resulted in hemorrhage. Furthermore, 8 of 19 esophageal injuries induced by aspirin were complicated by hemorrhage, compared to only one of five esophageal injuries caused by ibuprofen [7,8].
Endoscopy is the investigation of choice to document esophageal injury. However, it may not be necessary in all patients especially when history and temporal relationship is typical and other competing diagnosis are unlikely. It is indicated when the symptoms continue to progress or are inordinately persistent, when dysphagia predominates, or when the pill-taking history is not elicited. Endoscopy is also indicated by hemorrhage and in immunocompromised patients3. Junction of upper and middle third esophagus is most common site for mucosal injury due to anatomical narrowing of esophagus at this site. In one series, 80.0% of drug-induced esophageal ulcers were found in mid esophagus (28 to 33 cm from the incisors). Typically, ulcers are multiple, superficial and have flat edges. In this series mean number of drug-induced esophageal ulcers was 2.80 [9]. In our series all patients had ulcers in esophagus between 25 to 33 cm from incisor. Three patients had single ulcer and 14 had multiple, aphthous like ulcers of variable size. Biopsies are done only if there is suspicion of infection or neoplasia due to atypical or abnormal appearance of ulcers. We biopsied 4 ulcers to r/o other pathologies. One showed changes of acute esophagitis while three had nonspecific inflammatory changes. There was no suggestion of any inflammatory pathology or neoplasm on histology.
Treatment of drug induced esophageal ulcers traditionally includes stopping the offending agent, PPI, liquid antacids and soft diet. Most patients make quick recovery. We thought that one of the mechanisms involved in the pain is esophageal spasm in response to the mucosal injury. Secondly suppressing acid secretion for healing of ulcers located in mid esophagus looked too much of an extrapolation of assumption that these patients have severe reflux disease. Hence, we used either Nifedepine or Hyoscine butyl bromide which are esophageal smooth muscle relaxants along with topical anesthetic agent and alginate containing antacids or sucralfate. We did not use proton pump inhibitors in any patient. Our patients became asymptomatic within one week. Although we did not do a repeat endoscopy to document healing of the ulcers, it is not necessary in most of the patients and symptomatic relief can be equated with ulcer healing. All our patients were normotensive prior to starting these medications. None of them had any adverse event with either Nifedepine or Hyoscine butyl bromide. In our information, this is the first series in world literature which used Nifedepine or Hyoscine in pill esophagitis. We need to assess the efficacy of this approach in a randomized controlled trial as against the use of PPI.
Pill esophagitis is a potentially preventable adverse event of many medications. It can be prevented by
Spreading awareness about the possible medications capable of causing pill esophagitis so that medical practitioners prescribing these medications become aware of this complication. For this reporting and publication of data is particularly important.
Advising patients to consume potentially harmful medications with plenty of water and in upright position and to remain in upright position for at least 20 minutes after taking the pills. In my practice, I have tried a new approach of advising the patients to take the pills at the dining table just before starting the lunch or dinner so that the pill is flushed down the esophagus by the food. This has helped significantly and in my practice of more than 25 years, none of my patient reported symptoms of pill esophagitis after Doxycycline or NSAIDs.
Avoiding the use of potentially harmful medications in bed ridden, elderly, patients with pre-existing structural or functional disorders of esophagus.
Conclusions:
Pill esophagitis is an important, potentially preventable complication of many medications. It is often unrecognized, under reported entity. Odynophagia with temporal relationship to culprit medication is the hallmark of this disease. Usually it has self- limiting, benign course. Rarely it can be associated with complications like stricture, hemorrhage or perforation. Upper GI endoscopy is the investigation of choice. It can be reserved for atypical presentations, patients with possibility of competing diagnosis, patients with hemorrhage, strictures, or suspected neoplasia and for immuno-compromised individuals. Local anesthetic agents, Alginate containing antacid, sucralfate is often used along with proton pump inhibitors for treating these patients. For the first time in literature, we report successful use of Nifedepine and Hyoscine butyl bromide for relief of pain in these patients. This needs further randomized controlled trial. Patients should be advised to take medications with plenty of water or just before the meals and not to lie down for at least 20 min after taking any medication. Medical practitioners prescribing medications known to cause pill esophagitis should be made aware of this disease to improve awareness and for prevention of this disease.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org