Gastroenterology and Hepatology Research
OPEN ACCESS | Volume 7 - Issue 1 - 2026
ISSN No: 2836-2888 | Journal DOI: 10.61148/2836-2888/GHR


Lazaro Antonio Arango Molano, Md, FASGE1*, Andrés Sánchez Gil 2, Ileana Rocío Bautista Parada3, Claudia Patricia. Diaz T4
1General Surgeon, Clinical-Surgical Gastroenterologist, chief of gastroenterology program, Union de cirujanos SAS -Oncologos de occidente, Universidad de Caldas, Manizales, Colombia
2General surgeon, Clinical-Surgical Gastroenterologist, Union de cirujanos SAS -Oncologos de occidente,Universidad de Caldas, Manizales, Colombia.
3General surgeon, Clinical-Surgical Gastroenterology Fellow, Universidad de Caldas, Manizales, Colombia.
4General surgeon, Clinical-Surgical Gastroenterologist, Union de cirujanos SAS -Oncologos de occidente,Universidad de Caldas, Manizales, Colombia.
*Corresponding author: Lázaro Antonio Arango Molano, General Surgeon, Clinical-Surgical
Gastroenterologist, Universidad de Caldas, Manizales, Colombia.
Received date: March 22, 2021
Accepted date: March 30, 2021
Published date: April 02, 2021
Citation: Arango L A, Sanchez A, Bautista I R, Diaz CP (2021) Endosonographic Findings of Gastroduodenal Ectopic Pancreas: Experience of A Reference Center in Colombia and Literature Review. J Gastroenterology and Hepatology Research, 2(1); DOI: http;//doi.org/04.2021/1.1010
Copyright: © 2021 Lázaro Antonio Arango Molano, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background and aims: Ectopic pancreas (EP) is a congenital anomaly in which there is pancreatic tissue outside its usual anatomical location. Differentiating it from other subepithelial and tumor lesions is not easy, however, some typical endoscopic characteristics that allow a diagnostic approach with a high degree of accuracy have been described.
Materials and methods: We report a single-center retrospective study of consecutive patients who underwent to endoscopic ultrasonography between January 2016 and December 2019, as part of the study of gastric or duodenal subepithelial lesions and had findings consistent with ectopic pancreatic tissue.
Results: 23 patients were included, 15 women (65%) and 8 men (35%), the average age was 47 years (range 8-69 years); 19 were located in the antrum, 1 in the body-antral junction and 3 in the duodenal bulb. Central umbilication was identified in all cases. The average size of the lesions was 11 mm, the typical endosonographic "salt and pepper" pattern was identified in all cases, as an anechoic tubular structure (duct).
Conclusions: Typical endoscopic and endosonographic features are highly sensitive for the diagnosis of PE and include antral location, the presence of central umbilication, a long / short axis index> 1.5, submucosal location, mixed echogenicity, lobulated margins, absence of calcifications, and location between two or more sonographic layers.
Ectopic pancreas (EP), also called aberrant, heterotopic, or accessory, is a congenital anomaly in which there is pancreatic tissue outside its usual anatomical location. This tissue has no ductal, vascular, or neural connection with the main gland [1]. Multiple theories have been described about the origin of this condition, among which is the migration theory, in which it is proposed that fragments of pancreatic tissue separate from the developing pancreas during rotation of the foregut and are deposited in aberrant locations, the longitudinal growth of the intestine would also allow the pancreatic tissue to be located distally in some cases [2,3]. This theory would explain the predominant location of ectopic tissue in the upper gastrointestinal tract, since the pancreas develops from two primordia that originate from the foregut [4]. Other theories are metaplasia and the totipotent cells theory. According to the metaplasia theory, endodermal tissue migrates to the submucosa during embryogenesis and transforms into pancreatic tissue. In the totipotential cell theory, the endodermal cells that line the intestine differentiate into pancreatic tissue [5].The first case of heterotopic pancreas was described in an ileal diverticulum, a case published in 1729 by Jean Schulz. However, the first
Histological confirmation was made by Klob in 1859 [6].The true incidence of this condition is difficult to determine considering its generally asymptomatic course. It has been described in 0.5% of upper abdominal surgeries, in 0.55% -13.7% of autopsy series and in 0.9% of gastrectomies [7,8]. The presence of heterotopic pancreatic tissue in a Meckel diverticulum has been reported in 5 to 16% of cases [9].
Given the lack of information and studies of this condition in our population, the objective of this study was to describe the main endoscopic and endosonographic characteristics of patients treated in a referral center with endosonographic findings consistent with gastroduodenal ectopic pancreas.
Methods
A descriptive study was carried out with retrospective data collection. All patients treated at Union de Cirujanos (Gastroenterology Reference center located in Manizales / Colombia) from January 2016 to December 2019, who underwent endoscopic ultrasonography as part of the study of gastric or duodenal subepithelial lesions with findings consistent with ectopic pancreatic tissue were included in the study. Some of the patients underwent two or more endosonographic studies during the study period as part of the follow-up of the lesions, however,
for the data analysis, only the first studies carried out on each patient were included. A descriptive analysis of the registered data was carried out, the median was calculated for the numerical variables, while the qualitative variables were described with frequencies. Endoscopic ultrasound (EU) was performed using a Fujinon radial scanning endoscopic ultrasound equipment, SU-1 processor, high resolution, with variable frequencies of 7.5, 12 and 20 MHz, by three experienced gastroenterologists. All procedures were performed under intravenous sedation. Endosonographic characteristics were prospectively recorded for all lesions: location, central umbilication, maximum diameter, growth pattern, origin sonographic layer, echogenicity, presence of lobed margins and ductal structure. Based on the origin layer of the lesion, these were classified as superficial (second and / or third layer) or deep (third and / or fourth layer).
Results
23 patients were included, of which 15 were women (65%) and 8 men (35%), the average age was 47 years (range 8-69 years). Table 1. Regarding the lesions, 19 (19/23, 82%) were located in the antrum, 1 (1/23, 4%) in the body antral junction and 3 (3/23, 13%) in the duodenal bulb. Central umbilication was identified in 21 of the cases (91%). Figure 1.
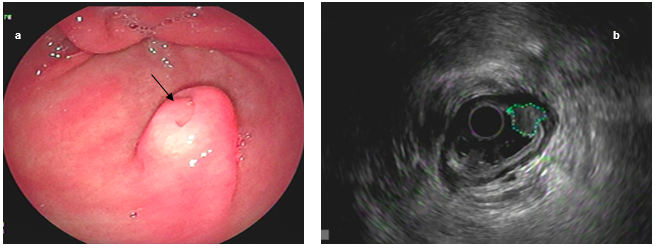
Figure 1. Antral ectopic pancreas with (a) central umbilication (arrow). Endosonographic appearance (b), delimited lesion (dotted line)
The average size was 11mm (range 5-19 mm) and the typical endosonographic pattern in “salt and pepper” was identified in all cases, as was the presence of an anechoic tubular structure (duct). Figure 2.

Figure 2. Antral ectopic pancreas (a). Endosonographic appearance (b), anechoic tubular structure, duct (arrow)
|
|
|||||||||||||||
|
Endosonographic Features |
|||||||||||||||
|
Case |
Gender |
Age |
Location |
Umbilication |
Size |
Growing |
Layer |
Echogenicity |
Lbulated |
Duct |
Sonographic |
||||
|
mm |
pattern |
margins |
Classification |
||||||||||||
|
1 |
F |
43 |
Antrum |
Absent |
11 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
2 |
F |
67 |
Antrum |
Absent |
17 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
3 |
F |
48 |
Antrum |
Present |
13 |
Intraluminal |
2,3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
4 |
M |
20 |
Antrum |
Present |
16 |
Intraluminal |
2,3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
5 |
F |
62 |
Antrum |
Present |
15 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
6 |
M |
54 |
Antrum |
Present |
9 |
Intraluminal |
3,4 |
Hyperechoic |
Present |
Present |
Deep |
||||
|
7 |
M |
52 |
Duodenum |
Present |
19 |
Intraluminal |
2 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
8 |
F |
47 |
Antrum |
Present |
10 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
9 |
M |
69 |
Antrum |
Present |
7 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
10 |
F |
67 |
Antrum |
Present |
17 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
11 |
M |
60 |
Duodenum |
Present |
7 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
12 |
M |
14 |
Antrum |
Present |
13 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
13 |
F |
64 |
Antrum |
Present |
18 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
14 |
F |
62 |
Antrum |
Present |
6 |
Intraluminal |
2,3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
15 |
F |
28 |
Antrum |
Present |
10 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
16 |
F |
67 |
Antrum |
Present |
10 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
17 |
M |
25 |
Antrum |
Present |
10 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
18 |
M |
8 |
Antrum |
Present |
8 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
19 |
F |
55 |
Antrum |
Present |
10 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
20 |
F |
55 |
Duodenum |
Present |
7 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
21 |
F |
35 |
Antrum |
Present |
10 |
Intraluminal |
2,3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
22 |
F |
62 |
Antrum |
Present |
5 |
Intraluminal |
3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
|
23 |
F |
28 |
Body – antrum junction |
Present |
9 |
Intraluminal |
2,3 |
Hyperechoic |
Present |
Present |
Superficial |
||||
Table 1. Clinical and endoscopic ultrasonography features of 23 patients with ectopic pancreas
In seventeen cases (74%) only the third sonographic layer was compromised, in six cases (26%) the second and third or third and fourth layers were involved (22% and 4% respectively). Figure 3.
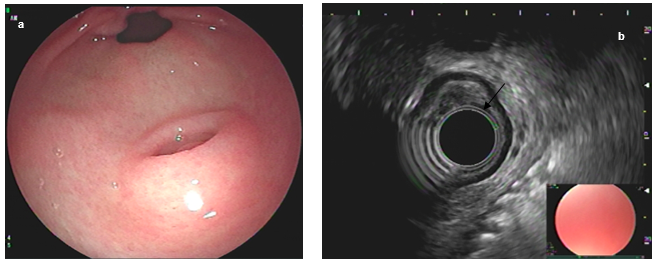
Figure 3. Antral ectopic pancreas (a). Endoscopic appearance (b), lesion involving the third sonographic layer (arrow).
95% of the lesions were classified as superficial and 5% deep. Clinical and endoscopic ultrasonography characteristics of all lesions are summarized in Table 2.
|
Feature |
|
|
N (%) |
|
|
Average age |
47.4 (8-69) |
|
||
|
Gender |
|
|||
|
Female |
15/23 (65%) |
|
||
|
Male |
8/23 (35%) |
|
||
|
Ubicación |
|
|||
|
Antrum |
19/23 (82%) |
|
||
|
Body |
1/23 (4%) |
|
||
|
Duodenum |
|
|||
|
Size |
|
|||
|
< o = 10 mm |
14/23 (61%) |
|
||
|
> 10, < o = 15 mm |
4/23 (17%) |
|
||
|
> 15 mm |
5/23 (22%) |
|
||
|
Umbilication |
|
|||
|
Present |
21/23 (91%) |
|
||
|
Absent |
2/23 (9%) |
|
||
|
Growing pattern |
|
|||
|
Intraluminal |
23/23 (100%) |
|
||
|
Ductal structure |
|
|||
|
Present |
23/23 (100%) |
|
||
|
EU classification |
|
|||
|
Superficial |
22/23 (96%) |
|
||
|
Deep |
1/23 (4%) |
|
||
|
Sonographic layer involved |
|
|||
|
2nd |
1/23 (4%) |
|
||
|
2nd and 3rd |
5/23 (22%) |
|
||
|
3rd |
16/23 (70%) |
|
||
|
3rd and 4th |
1/23 (4%) |
|
||
|
Lobulated margin |
|
|||
|
Present |
23/23 (100%) |
|
||
|
Ecogenicity |
|
|||
|
Hiperechoic |
23/23 (100%) |
|
||
|
Long/short diameter ratio |
|
|||
|
<1.5 |
10/23 (43%) |
|
||
|
|
>1.5 |
|
13/23 (57%) |
|
Table 2. Summary of clinical and Endoscopic ultrasonography features of ectopic pancreas
Discussion
EP can be located in any part of the gastrointestinal tract, most frequently it is located in the stomach (25% - 38%) and duodenum (9% - 36%). In the stomach, it is typically found in the antrum and prepyloric region, towards the greater curve (95% of cases) and posterior wall at an average distance of 3 to 6 cm from the pylorus. In the duodenum, lesions are usually located in the proximal segments [10]. In both the stomach and the duodenum, the lesions are generally round and ovoid [7,11]. The third most frequent location is the jejunum (0.5% - 35%), at this site, the lesions are usually smaller than 3 cm, flat and are generally located in the proximal jejunum, close to the Treitz ligament [2]. Lesions in the ileum correspond to 2.8% of cases. Ectopic pancreatic tissue has also been reported in the esophagus, where it is most frequently found in the distal third [12]. Other sites of unusual location are colon, cecal appendix, mesentery, liver, gallbladder, bile ducts, spleen, retroperitoneum, fallopian tubes, lungs, and mediastinum [4,13,14,15]. Macroscopically, the heterotopic pancreas is identified as a solitary, whitish or yellowish nodular lesion, which can vary in size from 0.5 to 5 cm [16]. Microscopically, heterotopic tissue is located in the submucosa, but in some cases, it can compromise all layers of the wall. (1) As reported in the literature, the most frequent location in this work was the gastric antrum, the average size of the lesions is also within the range described in previous studies.
Ectopic tissue can contain any mixture of the tissues normally found in the pancreas. In 1909 Heinrich described a classification of three histological types that was modified in 1973 by Gaspar-Fuentes adding a fourth histological type. There are to date 4 histological types of ectopic pancreas. Type I: composed of all the elements of the normal pancreas, Type II: composed only of pancreatic ducts (canalicular variety), Type III: composed of only acinar tissue (exocrine pancreas) and Type IV: composed only of cells of the Islets (endocrine pancreas) [10,17]. The clinical implication of the histological type in heterotopic pancreatic tissue or relationship with any specific pathology or laboratory findings has not been demonstrated so far [7,10].
In most cases, EP is asymptomatic and corresponds to an incidental finding in imaging and endoscopic studies performed for another reason. However, symptomatic cases also occur; more commonly in men between the ages of 40 and 50 [4]. Some patients may present with nonspecific symptoms such as abdominal pain, abdominal fullness, nausea, vomiting, anorexia, weight loss, anemia, or gastrointestinal bleeding. Abdominal pain is the most common symptom, generally secondary to irritation and inflammation of the surrounding tissues due to the secretion of pancreatic enzymes and hormones; It can also be the result of bleeding from the lesion due to erosion of the mucosa and formation of ulcers, especially in the small intestine; may therefore be a cause of hidden digestive bleeding [5,18]. Some patients may consult due to gastric outlet retention syndrome, especially in lesions greater than 2 cm located in the prepyloric region [1,7,19]. Symptoms usually depend on the location of the heterotopic tissue, size, or development of pathological changes similar to those that can occur in the pancreas (pancreatitis, cyst formation, or malignant transformation). Esophageal lesions can be the cause of dysphagia and epigastric pain, occasionally gastroesophageal reflux, nausea, and less frequently hematemesis [12]. In the jejunum, heterotopic tissue can act as the point of origin of an intussusception and if it is located in the ampulla it can lead to biliary obstruction [20,21].
Histological confirmation is the gold standard, however, due to the subepithelial nature of EP, conventional biopsies are only diagnostic in 10% of cases [1,22]. In this context, imaging and endoscopic findings are essential, even so, the diagnosis is not usually simple, considering that these are not completely specific. Despite advances in various diagnostic modalities, differentiation from other entities such as gastrointestinal stromal tumors remain a challenge. The main differential diagnoses include carcinoid tumors, gastrointestinal or mesenchymal stromal tumors such as leiomyomas or neurofibromas, lymphoma, and gastric carcinoma [4].
On upper gastrointestinal radiography, the heterotopic pancreas usually has a broad base and a smooth surface; occasionally they can appear as sessile lesions with a narrow base and can be confused with polyps. Central umbilication can be identified by accumulation of barium in the center of the lesion and corresponds to the ductal remnant, this image suggests the diagnosis of heterotopic pancreatic tissue, however, large umbilications can correspond to ulcers that in turn can be benign or correspond to ulcerated tumor lesions [20].
In computed tomography, heterotopic pancreatic tissue is usually identified as an oval intramural lesion, with ill-defined or micro lobulated borders [2,5]. They are generally small lesions, less than 3 cm and with an endoluminal growth pattern [23]. Attenuation and enhancement characteristics depend on their histological type. Those lesions mainly composed of acini show homogeneous enhancement that can be equal to or greater than that of the pancreatic gland and greater than that of other types of PE. Those that are mainly composed of ductal structures present hypo enhancement and are sometimes surrounded by hypertrophic muscle [5,24]. Some tomographic findings have been described that allow the differentiation of gastric and duodenal heterotopic pancreatic tissue from gastrointestinal stromal tumors and other lesions with a high degree of accuracy, these are: the predominant antral location, poorly defined borders, prominent enhancement of the overlying mucosa, long / short diameter ratio greater than 1.5, and an endoluminal growth pattern [25]. Unlike ectopic tissue located in the stomach or duodenum, in the jejunal ectopic pancreatic tissue, central umbilication or enhancement of the overlying mucosa is not usually identified, nor has a dominant growth pattern been described, some criteria have been proposed to differentiate these lesions from submucosal tumors: flat shape, presence of micro lobulations and a structure similar to a duct within the lesion, mainly if it is located in the longitudinal axis of the lesion [2].
On magnetic resonance, the appearance of the EP emulates orthotopic pancreatic tissue. The elevated signal intensity on T1 is particularly useful in differentiating the ectopic pancreas from other lesions. Magnetic resonance cholangiopancreatography can help identify the rudimentary ductal system; a finding highly suggestive of EP [20].
The typical endoscopic characteristics are lesions with a broad base, round or oval shape, submucosal location, 3-6 cm proximal to the pylorus at around 5 o'clock, and the presence of central umbilication, however, this last finding can also be identified in submucosal neuroendocrine tumors and hamartomas [10,1]. It has been reported that the use of magnification endoscopy with narrow band imaging allows the identification of the microscopic pancreatic duct on its surface, a finding that could be useful in the differentiation of other subepithelial lesions [26].
EU is perhaps the most useful tool in the characterization of subepithelial lesions; however, it cannot determine whether these correspond to benign or malignant lesions with absolute certainty. The EU provides the most accurate information regarding the
location within the gastric wall [27]. EP can be located in any of the layers of the gastrointestinal tract wall, it is located mainly in the submucosa (75%) and sporadically in the muscularis propria (17%), mucosal and serous involvement are rare [28]. The sensitivity of EU for the diagnosis of EP has been reported between 84.6 and 90% [22,29]. Mixed echogenicity, indefinite borders, absence of calcifications, and location between two or more layers have been described as typical endosonographic characteristics, all of which were present in 100% of the cases included in this study. The presence of central umbilication has been described in up to 50% of the cases [30,31]. however, in our case central umbilication associated with the presence of a ductal structure was found in 91% of the lesions. EP can be endosonographically classified into two types: superficial and deep, superficial are those lesions that compromise only the second and / or third layer and deep are those that compromise the fourth layer or exceed it, in this study only 4% of cases had involvement of the fourth layer [29,32,32]. The long axis / short axis ratio> 1.5 has been described as a highly suggestive characteristic of EP and that would also allow it to be differentiated from gastrointestinal stromal tumors (GIST) [22]. although only 56% of the lesions described in this study had an index> 1.5, all the cases presented both the typical echogenic pattern of "salt and pepper" and an associated ductal structure.
Taking into account the high diagnostic sensitivity of the EU, it is suggested that the biopsy be performed only in the case of homogeneous-hypoechoic lesions that compromise the muscularis propria and have a long / short axis index > 1.5, seeking to differentiate EP type deep from other hypoechoic subepithelial lesions such as leiomyomas, GIST, inflammatory polyps or Schwannomas, the yield of this biopsy has been reported between 60% and 78.4 %% [22,29,33,34].
Among the complications of ectopic pancreatic tissue, gastric outlet retention syndrome, ulceration, intestinal perforation, and digestive bleeding have been described [35]. Cystic dystrophy is an unusual but serious complication, which corresponds to the dilation of the pancreatic ducts ectopic. Cases of acute and chronic pancreatitis and pseudocysts originating in ectopic pancreatic tissue have also been reported[8,17]. Malignant transformation is rare and occurs mainly towards adenocarcinoma, to date there is only one report of neuroendocrine carcinoma originated in pancreatic ectopic tissue [36].
To date, there are no treatment guidelines for this condition, however, three management options have been proposed: surgical resection, endoscopic resection, or endoscopic follow-up. It is accepted that asymptomatic patients with lesions smaller than 2 cm do not require specific treatment and can be followed endoscopically, it is suggested that the endoscopic follow-up be performed in less than 2 years with respect to the initial study, however, the duration of follow-up is not good established. Other authors propose, considering the potential risk of malignant transformation, the resection of lesions > 1cm or when there is ulceration, secondary obstruction, or weight loss [8].
Laparoscopic resection has proven to be an effective and safe method for EP resection [37]. however, it is not without complications and has limitations when the lesions are located near or in the pyloric canal. Endoscopic submucosal dissection, meanwhile, is a feasible and safe option, which can be considered even in duodenal lesions and has ana bloc resection rates of up to 100% [38,39,40].
Conclusion
Even though this is a retrospective study, the number of patients included is small and there is no histological confirmation, it can be concluded that typical endoscopic and endosonographic features are highly sensitive for the diagnosis of PE and include antral location, the presence of central umbilication, a long / short axis index> 1.5, submucosal location, mixed echogenicity, lobulated margins, absence of calcifications, and location between two or more sonographic layers. Clinical follow-up is an option in asymptomatic patients with lesions that lack endosonographic features suggestive of other subepithelial lesions.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org