Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Suriyaprakash Nagarajan
Department of Radiodiagnosis, Government Kilpauk Medical College Hospital, Chennai, Tamil Nadu, India.
*Corresponding author: Suriyaprakash Nagarajan, Department of Radiodiagnosis, Government Kilpauk Medical College Hospital, Chennai, Tamil Nadu, India.
Received: September 08, 2021
Accepted: September 20, 2021
Published: September 22, 2021
Citation: Suriyaprakash Nagarajan “Lipodystrophy - Can the radiologist give a clue to the diagnosis?.” Clinical Case Reports and Clinical Study, 5(4); DOI: 10.61148/2766-8614/JCCRCS/092
Copyright: © 2021 Suriyaprakash Nagarajan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
,
Introduction:
Lipodystrophies are a heterogeneous group of disorders characterized by selective deficiency of adipose tissue or abnormal disposition of fat in the absence of nutritional deprivation or catabolic state [1]. Lipodystrophy presents with unilateral limb thinning with normal clinical, physical and nerve conduction studies. Most common cause of unilateral limb thinning is monomelic amyotrophy, which is a motor neuron disease with muscle atrophy without pain or sensory loss. There is no definite cure for monomelic atrophy except for spinal surgery in advanced cases. It is crucial to differentiate lipodystrophy from amyotrophy, as the former can be managed conservatively. We report a case of 10-year-old girl presenting with unilateral limb thinning.
Case report:
A 10 year, second born girl child of non-consanguineous marriage was brought by her mother with history of thinning of right lower limb (Figure 1) over a of 6 months. The patient neither had weakness, pain, cramps, fasciculation or sensory involvement nor significant past history of trauma or medication for chronic illness. Birth history of the child was uneventful. She had normal developmental milestones. No similar complaints in any other family member or sibling.

Figure 1: Unilateral thinning of right lower limb.
Physical examination revealed thinning of right lower limb and right anterior chest wall (Figure 2). Skin over the lower limb and chest appeared normal. Neurological examination did not show any deficit and power was normal in both proximal and distal group of muscles in both lower limbs, with preserved reflexes and sensation.

Figure 2: Right anterolateral chest wall appears hollow. No clinical complaints.
Electromyography of both lower limbs was normal. Evaluation for lipodystrophy related conditions like blood glucose level, lipid profile and HIV status were normal. MRI of whole spine was essentially normal. MR evaluation of the lower limbs showed subcutaneous lipoatrophy of the right lower limb predominantly involving upper thigh with preserved fatty marrow and muscle mass (Figure 3). MR evaluation of thorax showed subcutaneous lipoatrophy in right pectoral region with preserved muscle mass (Figure 4).
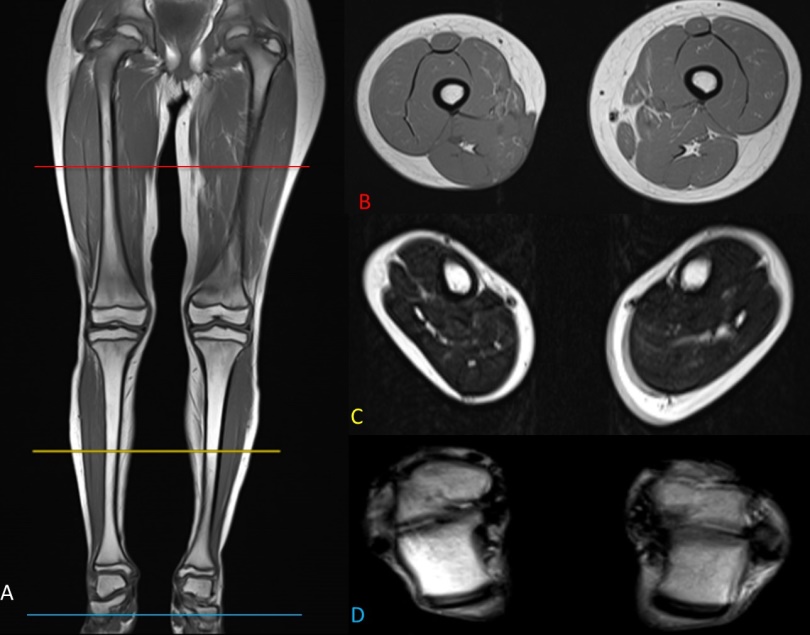
Figure 3: Coronal non-FS MR of both lower limbs shows the loss of subcutaneous fat in right lower limb with normal muscle mass and bone marrow. B(red), C(yellow) and D(blue) shows axial images at thigh, mid-calf and ankle level respectively showing atrophy of subcutaneous fat at these levels.
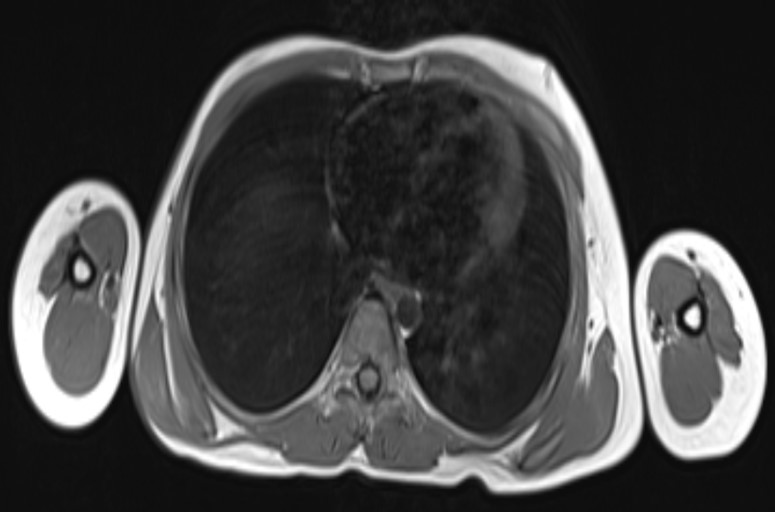
Figure 4: Axial non-FS MR image shows loss of subcutaneous fat in right anterior chest wall.
Clinical follow up of the patient done after 6 months showed no progression or further thinning. The clinical presentation, the laboratory investigations, natural course and radiological imaging in the patient has given the diagnosis of sporadic case of partial lipodystrophy involving right lower limb and anterior chest wall. Genetic testing was not carried out in this patient as the patient did not show clinical progression and genotyping is usually indicated only in patients with positive family history.
Discussion:
Lipodystrophy is an idiopathic systemic disorder characterized by atrophy of adipose tissue or abnormal disposition of fat. Lipodystrophies can be categorized according to the etiology as genetic or acquired and based on distribution of loss of adipose tissue as generalized, partial or localized [1]. Generalized lipodystrophy is characterized by near total loss of subcutaneous adipose tissue. Partial lipodystrophy is selective loss of adipose tissue. Localized lipodystrophy is defined as loss of fat at localized site like insulin injection sites. Leptin, adipocyte hormone plays an important role in maintaining the adipocyte mass and its deficiency may lead to lipodystrophy and other metabolic abnormalities [2]. The atrophy of fat tissues may be associated with hypertriglyceridemia, insulin resistance and metabolic syndrome. Associated metabolic, autoimmune, and renal disease and HIV infections have to be ruled out. Role of MR imaging in lipodystrophy is to evaluate the fat loss or abnormal accumulation. No definite diagnostic criteria for lipodystrophy have been established based on skinfold measurements or imaging modalities like magnetic resonance imaging [3].
Acquired partial lipodystrophy typically involves the face extending to thorax and upper limbs. Rarely, there can be acquired lipodystrophy involving one lower limb. Idiopathic localized
lipodystrophy is a lipodystrophy condition due to undetermined etiology.
The possible differential diagnosis to be considered includes conditions presenting with severe weight loss like malnutrition, anorexia nervosa, thyrotoxicosis and chronic infection. These conditions will be evident by widespread involvement with muscle mass decrement and other associated clinical features.
Usefulness of MRI in the diagnosis of lipodystrophy is to evaluate loss or abnormal accumulation of subcutaneous fat and assess the bone marrow and muscle mass. The classic MRI finding in lipodystrophy includes loss of fat in T1 sequence, with preserved marrow fat and muscle fat [4].
Treatment of lipodystrophy is focused on managing the metabolic abnormalities to prevent complications, and aesthetic purpose [5]. Diet and exercise form an integral part of the treatment plan.
Conclusion:
Lipodystrophies are a heterogeneous group of disorders with diverse pathophysiology. For diagnosis, clinical suspicion and physical examination are critical. Recognition of imaging findings associated with lipodystrophy is essential in order to make an accurate diagnosis. Improving the detection of lipodystrophy and increasing general awareness of the disease will help to ensure that patients with lipodystrophy receive appropriate treatment.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org