
Alberto Monello 1*#MD, Giorgio Benatti 2*MD, Luciano Losi 1MD, Iacopo Tadonio 2MD, Vincenzo Guiducci 3MD, Daniela Aschieri 1MD, Luigi Vignali 2MD, PhD.
1 Division of Interventional Cardiology, Ospedale Guglielmo da Saliceto, Azienda Unità Sanitaria Locale di Piacenza, Italy;
2 Division of Interventional Cardiology, Ospedale Maggiore, Azienda Ospedaliera Universitaria di Parma, Italy;
3 Division of Cardiology, Arcispedale Santa Maria Nuova, Azienda Unità Sanitaria Locale IRCSS di Reggio Emilia, Italy.
*Corresponding author: Alberto Monello, MD, Division of Interventional Cardiology, Ospedale Guglielmo da Saliceto, Azienda Unità Sanitaria Locale di Piacenza Via Giuseppe Taverna, 49, 29121 Piacenza (PC), Italy
*The first two authors contributed equally and should be considered co-first authors
Received: September 11, 2023
Accepted: September 20, 2023
Published: September 22, 2023
Citation: Monello A, Benatti G, Losi L, Tadonio I, Guiducci V. (2023) “Accidental Balloon Misalignment During Edwards Sapien 3 Ultra Transcatheter Heart Valve Implantation.” J Clinical Cardiology Interventions, 3(2); DOI: http;//doi.org/10.2023/07.1041.
Copyright: © 2023 Alberto Monello. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
We herein describe a case of accidental balloon misalignment during Edwards Sapien 3 Ultra Transcatheter Heart Valve implantation and the technique used to overcome this undesirable situation and successfully deploy the valve.
Introduction
Inattentive errors during preparation of a Transcatheter Heart Valve (THV) are rare occurrences, but when they occur their handling may pose major challenges and potentially lead to dreadful consequences.
Case Report
An 82-year-old gentleman presented to our department for evaluation of new-onset exertional angina and dyspnea. His pertinent comorbidities included hypertension, dyslipidaemia, type 2 diabetes, obesity (body mass index 31), persistent atrial fibrillation on oral anticoagulation and previous carotid percutaneous transluminal angioplasty. Transthoracic echocardiography showed reduced left ventricular ejection fraction (EF 42%) and severe aortic stenosis (mean transvalvular gradient 37 mmHg, aortic valve area 0.76 cm2). Coronary angiography revealed significant two-vessel disease involving the proximal left anterior descending artery (LAD) and mid left circumflex artery (LCX). After Heart Team discussion (≥ 75 years, EuroSCORE II 4,71%) and coronary revascularization (a drug-eluting stent was deployed to the LAD and drug-coated balloon to LCX), the patient underwent Transcatheter Aortic Valve Implantation (TAVI) with 26 mm Edwards SAPIEN 3 Ultra (S3U) THV. During the alignment of the valve, fine adjustment wheel was inadvertently overturned past the distal marker ending up with a major distal misalignment of the THV over the balloon. As known, it was not possible to retrieve the valve in the correct position at that point. We balanced the risks related to the retrieval of the system throug the eSheath (Edwards Lifesciences) with the valve in that position and the risks of proceeding with the implantation. After discussion with the team, a decision was made to try to deploy the misaligned THV. After crossing the aortic valve (Figure 1B, Video 1), an attempt was made to partially open the prosthesis, with the aim to engage the deflated balloon in a more proper position and fully deploy with a second step full expansion. However, initial opening of the shoulder of the balloon made it slip even more proximally while expanding the THV only in the outflow part in a “frightening conic shape” (Figure 1C and 1D, Video 2). Luckily, under uninterrupted rapid pacing of about 40-45 seconds, it was possibile to dilate the inflow part of THV with a slow dilatation of the balloon while applying firm pushing force on the delivery system (Figure 1E and 1F, Video 2). Another inflation was performed (with overfilling with 2 ml above the nominal volume) to achieve full expansion and a proprier shape of the THV with very good angiographic result (Figure 1G; Video 3). The procedure was performed successfully, with no major complications, no aortic regurgitation, no conduction disturbances and patency of both coronary arteries. Echocardiogram showed unremarkable mean gradient, no paravalvular leaks and improved left ventricular systolic function (EF 53%). Postprocedural course was uneventful and the patient was discharged to home 2 days after the procedure.
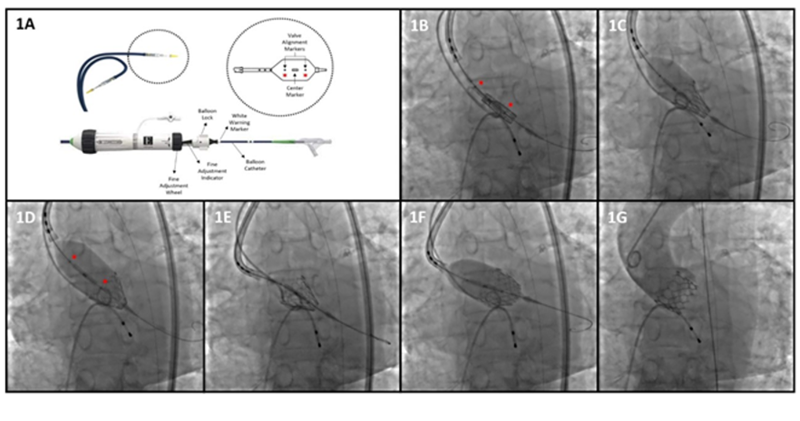 Figure 1: (1A) Edwards Commander delivery system. (1B) S3UTHV across aortic valve with balloon markers (red dots) showing misalignment. (1C) First balloon inflation (1D) expanding only the outflow part. (1E) Pushing force applied on the delivery system to maintain the deflated balloon in contact with S3UTHV. (1F) Second balloon inflation with opening of the inflow part. (1G) Final result after third balloon inflation.
Figure 1: (1A) Edwards Commander delivery system. (1B) S3UTHV across aortic valve with balloon markers (red dots) showing misalignment. (1C) First balloon inflation (1D) expanding only the outflow part. (1E) Pushing force applied on the delivery system to maintain the deflated balloon in contact with S3UTHV. (1F) Second balloon inflation with opening of the inflow part. (1G) Final result after third balloon inflation.
Video 1. SAPIEN 3 Ultra Transcatheter Heart Valve (S3U THV) across aortic valve with balloon markers showing gross misalignment.
Video 2. Initial first balloon inflation expanding only the outflow part of the THV in a conic shape followed by pushing force applied on the delivery system to maintain the deflated balloon in contact with the inflow part and second balloon inflation with proper opening of the inflow part of S3U THV.
Video 3. Final result after third balloon inflation.
Discussion
To the best of our knowledge, this is the first case reporting successfull implantation of an accidentally misaligned S3U THV during loading manoeuvres over the balloon. Surely, it should be stressed that it is paramount to maintain adequate attention to all stages of valve preparation and procedural steps. We carefully discussed pros and cons, but the final decision was to proceed with the implantation, also due to the absence of high-risk anatomical factors that could have impaired the multi-step deployment (coronary artery ostia height, degree of calcification, size of the sinus of Valsalva/ascending aorta/left ventricular outflow tract). We can summarize the procedure in three steps: 1) first inflation expanding only the outflow part of the THV; 2) pushing force applied on the delivery system to maintain the deflated balloon in contact with the inflow part and second balloon inflation with opening of the inflow part of the THV; 3) final inflation to optimize the result. However, though we describe a possible bail-out technique to overcome this unexpected event, it must be emphasized that for safety reasons THV deployment should not be attempted when facing this deprecable situation.
Conclusion
We described an accidental balloon misalignment during fine adjustment of Edwards SAPIEN 3 Ultra Transcatheter Heart Valve and the bail-out technique used to overcome this unexpected event; however, before proceeding with the implantation, careful balancing of benefits and risks should be undertaken, and safety should always be prioritized.
The Authors declare that there is no conflict of interest.
Relationship with industry and financial disclosure statement: none.
Institution where the procedure was performed: Division of Interventional Cardiology, Ospedale Maggiore, Azienda Ospedaliera Universitaria di Parma, Italy.
,

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org