
Toure M1,2,6, Dagnogo M1, Terra A W1, Djiguiba K5, Doumbia M4, Ba Ho2,6, Konate M6, Fofana D1, Diall A.A1, Diarra B2, Sow M1, Daffe S1, Thiam C A1,6, Keita A1,6, Coulibaly M1, 5, Sangare A3, Diarra B I 4, Diakite M 3,6, Coulibaly S M1, Sankare H 1, Diarra Mb 1,6, Menta I 2,6
1Cardiology Department, CHU- Mère Enfant, Bamako-Mali.
2Cardiology Department, CHU-Gabriel Touré, Bamako-Mali.
3Cardiology Department, CHU-Point G, Bamako-Mali.
4Center Andre FESTOC, Department surgery cardiac of Bamako Mali.
5Nephrology - Hemodialysis - Peritoneal Dialysis - Renal Transplantation, CHU- Mère Enfant, Bamako-Mali.
6Faculty of Medecine, University Sciences Technic and Technology of Bamako
*Corresponding Author: Mamadou TOURE, Cardiology Department, CHU- Mère Enfant. Bamako Mali.
Received date: October 22, 2022
Accepted date: November 07, 2022
published date: January 31, 2023
Citation: Toure M, Dagnogo M, Terra A W, Djiguiba K, Doumbia M. (2023) “The Stenting of aneurysm of the anterior interventricular artery (AIV) in a case report from Mali.” J Clinical Cardiology Interventions, 3(1); DOI: http;//doi.org/10.2023/1.1030.
Copyright: © 2023 Mamadou TOURE. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Coronary aneurysm is defined by a coronary dilatation to more than 1.5 times the diameter of the artery concerned. It is a rare condition with an overall prevalence ranging from 0.2 to 6% with a male predominance. The two main causes are inflammatory diseases and atheromatous etiology. The two main causes are inflammatory diseases and atheromatous etiology. We report the case of a 60-year-old hypertensive patient admitted to the cardiology department for constrictive chest pain. He was admitted to the KT ward where coronary angiography showed an anterior interventricular artery (IVA) aneurysm successfully treated with a covered stent.
Introduction
Coronary aneurysm is defined as a coronary dilatation to more than 1.5 times the diameter of the involved artery [1-3]. It was first described by Charles Bougon in 1812 [4]. It is a rare condition with an overall prevalence ranging from 0.2 to 6% with a male predominance [1,2, 5]. The two main causes are inflammatory diseases and atheromatous etiology [2,6]. The aneurysm can be fusiform or saccular. We report the case of an aneurysmal lesion of the anterior interventricular artery successfully treated with a covered stent.
Observation
Mrs BD., 60 years old with cardiovascular risk factors, dyslipidemia and hypertension, was admitted to the catheterization room for prolonged constrictive chest pain and stage III dyspnea, which had not been relieved by a doliprane 1000 tablet and two puffs of sublingual trinitrine and had been evolving for several days. The clinical examination on admission noted a precarious hemodynamic state with a BP of 95/60mmhg, a SaO2 of 85%, a HR of 124 bpm, irregular heart sounds, rapid without abnormal noises, and crepitating rales at both lung bases. The ECG shows atrial fibrillation, right bundle branch block and diffuse ST segment elevation (Fig.1).
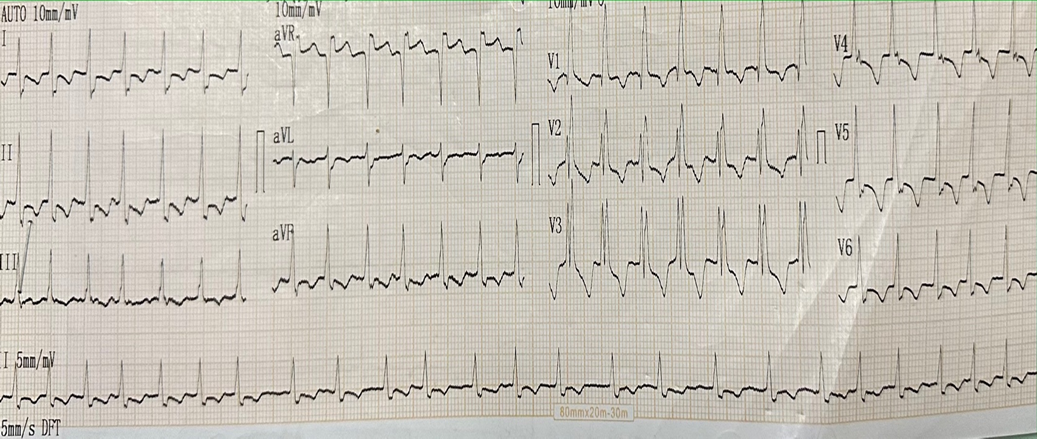
Figure 1 : Atrial fibrillation, right bundle branch block, ST segment overshift in Apr., diffuse ST segment undershift.
ETT shows minimally reduced LV systolic function, EF at 40-45%, global Hypokinesis especially inferior and apical-lateral.
Coronary angiography performed via the right radial approach shows tri-truncular lesions with significant stenosis of the right coronary (Fig.2),
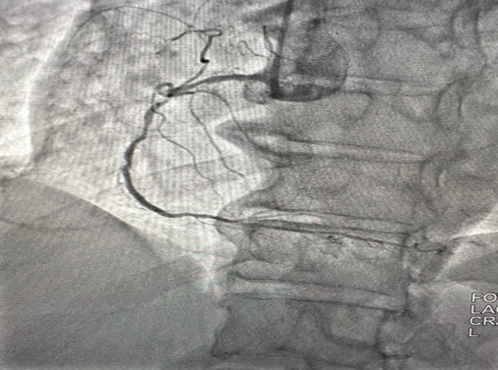

Figure 2 : Staggered stenosis of the right coronarysignificant stenosis of the middle circumflex and significant stenosis of the proximo-medial anterior interventricular which is also the site of a saccular aneurysm (Fig.3).
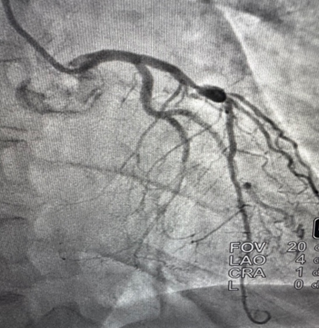

Figure 3 : Significant middle circumflex (Small arrow) and middle anterior interventricular stenosis with aneurysm (Large arrow).
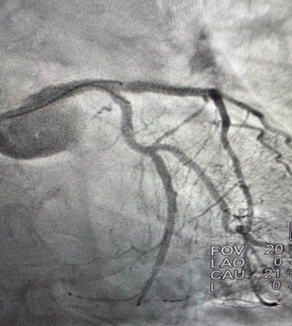
Figure 4: Successful angioplasties of the middle circumflex and middle anterior interventricular with aneurysm exclusion.
The patient was successfully treated with a Graftmaster 2.75/28 mm covered stent to exclude the aneurysm and the circumflex artery with an Ultimaster 2.5/34 mm active stent.
Follow-up was simple, allowing discharge after one week of observation with acetylsalicylicacid, clopidogrel, rivaroxaban, atorvastatin, bisoprolol and perindopril.
Discussion
The mode of revelation of coronary aneurysms is varied, from chronic coronary syndrome to acute coronary syndrome via silent ischemia, in our patient it was during an acute coronary syndrome. [7]
Atherosclerosis is the most common cause of coronary aneurysms and we believe that this is the case in our patient considering the atheromatous involvement of other arteries. [2, 6,7]
The classic cardiovascular risk factors are usually found with a high prevalence of smoking in the literature, however our patient was not a smoker but had hypertension, dyslipidemia and her age as cardiovascular risk factors. [8,9]
Coronary angiography is the reference examination for the diagnosis of coronary aneurysms, as in our patient. [7,10]
The right coronary artery is the preferred location for coronary aneurysms but in our patient it was the anterior interventricular artery. [10, 11,12]
The treatment of aneurysms depends on the size, can be surgical especially for giant aneurysms, which can combine repair or exclusion of the aneurysm and coronary artery bypass surgery
[1, 3,7] Coronary angioplasty can be an alternative to surgery as in our patient. [13,14]
The use of the covered stent allowed us to successfully treat both the VIA stenosis and exclude the aneurysm in our patient.
Conclusion
Covered stents are an alternative to surgery for the management of coronary aneurysms. However, their use probably requires long-term double antiaggregation because we had no experience with their risk of thrombosis.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org