
Laxminarayan Sarbere 1*, Sadik Khan 2, Preeti Sarbere 3
1Clinic Head, Tukum, Chandrapur
2Zonal Medical Head of Pune and Vidarbha Region,Madhavbaug Cardiac Clinic and Hospital,Thane
3Clinic Head, Jatpura Gate, Chandrapur
*Corresponding Author: Laxminarayan Sarbere, Clinic Head, Tukum, Chandrapur.
Received date: September 26, 2022
Accepted date: October 21, 2022
published date: October 31, 2022
Citation: Laxminarayan Sarbere, Sadik Khan, Preeti Sarbere. (2022) “To Study Efficacy of Ischaemia Reversal Programme (Irp) In Stable Ischaemic Heart Disease (Ihd) Patients to Improve Quality of Life.” J Clinical Cardiology Interventions, 2(5); DOI: http;//doi.org/10.2022/1.1029
Copyright: © 2022 Laxminarayan Sarbere. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Context: Despite the existence of comprehensive recommendations for the care of IHD and HTN, the frequency of IHD is increasing. For the treatment of IHD with HTN, the ischemia reversal programme (IRP) combines Panchkarma with nutrition therapy.
Aims: The current study was done to evaluate the impact of IRP in patients with IHD and HTN in terms of maximal oxygen uptake and maximum aerobic capacity as determined by VO2max (V-volume, O2-oxygen, max-maximum), Duke's treadmill score (DTS), diastolic BP (DBP) and systolic (SBP).
Settings and Design: The current study was a record-based retrospective cohort study done at Madhavbaug clinic Chandrapur, Maharashtra.
Methods and Material: Regardless of gender, we included patients in the age group 40-75 years with diagnosis of IHD and coronary artery disease. Baseline measurements of body weight, body mass index (BMI), abdominal girth (ABG), DTS, SBP, DBP on day 1 and day 90 of IRP were noted.
Statistical analysis used: Paired t-test was used to analyze the difference in various parameters at baseline and completion of therapy i.e. 90 days.
Results: On analyzing the various parameters, it was found that weight, abdominal girth, glycosylated hemoglobin, body mass index, systolic blood pressure and diastolic blood pressure showed statistically significant improvement at day 90 as compared to day 1. Mean Dukes treadmill score at day 1 was -1.76, whereas day 90 mean reading of Dukes treadmill score was found to be 6.34.
Conclusions: After IRP, there was a noticeable improvement in VO2max, Duke's treadmill score, SBP, and DBP indicating its beneficial role in IHD with HTN.
Introduction: In both emerging and industrialized nations, the incidence rates of the two main cardiovascular diseases (CVDs), ischemic heart disease (IHD) and hypertension (HTN), have risen to epidemic proportions. According to a global analysis, these estimates have resulted in 18 million fatalities. The results of several research have confirmed that HTN is a significant traditional risk factor for IHD in a wide range of populations throughout the world. The hypothesis that HTN may enhance IHD through a shared pathophysiology with atherosclerosis, namely oxidative damage and arterial wall inflammation, is supported by this epidemiological observation. It is anticipated that IHD and HTN will be responsible for more than 80% of CVD-related fatalities. In India, the prevalence of sedentary lifestyles is increasing due to habitual inactivity and obesity, which has raised morbidity and mortality from illnesses including IHD, HTN, diabetes, abnormal cholesterol levels, etc. Over the past 20 years, there has been a significant increase in the number of deaths related to IHD alone.1
Despite the fact that there are affordable therapeutic options available in India, the best use of these resources has been hindered by a number of factors including low disease awareness among the general inhabitants, minimal diagnosis levels, reduced adherence rates, and low use of evidence-based therapeutic options. Despite the existence of comprehensive recommendations for the care of IHD and HTN, the frequency of IHD is increasing.2 Additionally, there is a complicated interplay between several parameters, such as age, concomitant illnesses, other drugs, etc., in the treatment of IHD. Therefore, it is crucial that we investigate novel treatment alternatives that will aid in restoring normalcy to the quality of life by lowering anxiety and dread in patients with IHD and HTN.2
Traditional medications used to treat IHD with HTN work by lowering blood pressure (BP), keeping the heart's oxygen demand and supply in balance, having an antioxidant impact, bringing elevated lipid levels back to normal, and preventing platelet aggregation. These medications can quell the exploratory search for a novel therapeutic option for the management of IHD patients because analogous activity has been discovered in a variety of herbal medications in clinical studies.3,4 Panchkarma, a multi-step treatment for internal body purification, is recommended in the chronic phase of disease according to Ayurvedic Science of Medicine.
For the treatment of IHD with HTN, the ischemia reversal programme (IRP) combines panchkarma with nutrition therapy. The three procedures employed in panchkarma, which is a programme widely used for bodily purification, are snehana, or therapeutic oleation, swedana, or passive heat treatment, and basti, or therapeutic enema.5 Given that HTN and IHD are strongly related with sadness, a diminished sense of inner strength, a decreased quality of life, and anxiety,5 we designed the current study to evaluate the impact of IRP in patients with IHD and HTN. We looked at how IRP affected the maximal oxygen uptake and maximum aerobic capacity as determined by VO2max (V-volume, O2-oxygen, max-maximum), Duke's treadmill score, diastolic BP (DBP) and systolic (SBP), as well as the dependence of these IHD patients on normal conventional drugs.
Subjects and Methods: The current study, which covered the period from March 2018 to December 2021, was a record-based retrospective cohort study. The study was conducted at Madhavbaug clinic Chandrapur, Maharashtra. Regardless of gender, we included patients in the age group 40-75 years with diagnosis of IHD and coronary artery disease. Records of patients with recent history of myocardial infarction in previous 3 weeks before admission, unstable angina, severe hepatic or renal insufficiency, acute heart failure, severe aortic stenosis, cardia arrythmia, severe anemia and pregnant and lactating patients were excluded from the study.
Baseline measurements of body weight, body mass index (BMI), abdominal girth (ABG), Duke's treadmill score (DTS), Systolic blood pressure (SBP), diastolic blood pressure (DBP) on day 1 of IRP were noted. On day 90 of IRP, same procedure was repeated in order to determine the percent change from the baseline value. The percentage of patients out of the total recruited patients who needed a traditional allopathic therapeutic agent over the trial term of 90 days was used to calculate the reliance on standard medicine both on day 1 and day 90 of IRP.
The formula used to compute DTS is as follows6:
Duke treadmill score = Total MET - (5 x ST segment deviation (in mm)) – (4 x angina index)
where 0 indicates no angina, 1 indicates non-limiting angina, and 2 indicates exercise-limiting angina
Out of the patients described above, those who received IRP for at least 7 sittings during a period of 90–15 days were chosen for study. Finally, only those patients were counted who had full patient information from day 1 to day 90 of IRP available from Madhavbaug clinics' outpatient departments in cities throughout the state of Maharashtra.
Medical records show that patients were instructed to consume a light meal before beginning a three-step IRP. One session took 65 to 75 minutes to complete, as shown in table 1.2
|
Table 1: Study Treatment: Ischemia Reversal Program (IRP Kit) |
|||
|
Step of IRP |
Type of Therapy |
Herbs used for therapy |
Duration of Therapy |
|
Snehana |
Massage or external oleation (centripetal upper strokes directed towards heart) |
100 ml [Sesame oil (80%) + Lavender oil (20%)] |
30-35 minutes |
|
Swedana |
Passive heat therapy |
Dashmoola (group of ten herbal roots) with steam at < 40 degrees Celsius) |
10-15 minutes + 3 - 4 minutes of relaxation after procedure |
|
Basti |
Per rectal drug administration using a rectal solution. |
Luke-warm GHA decoction 100 ml |
15 minutes |
Statistical analysis: In a Microsoft Excel spreadsheet, data were collected and coded. Software R 3.4.4 was used to evaluate data. Continuous data were reported as the Mean SD, whereas categorical data were shown in frequency form. Paired t-test was used to analyze the difference in various parameters at baseline and completion of therapy i.e. 90 days. p-value <0.05 was considered as statistically significant.
Results: Out of 40 patients, mean age was 55.1 ± 7.35 years. On gender analysis, majority of the patients were males comprising of 25 patients (63%), while 15 (37%) patients were females [table 2].
|
Sr. No. |
Category |
Sub-category |
n (%) |
Mean ± SD |
|
1 |
Age |
|
|
55.1 ± 7.35 |
|
2 |
Gender |
Male |
25 (63%) |
|
|
Female |
15 (37%) |
|
Table 2: Demographic details of the patients in the present study.
On analyzing the various parameters, it was found that weight, abdominal girth, glycosylated hemoglobin, body mass index, systolic blood pressure and diastolic blood pressure showed statistically significant improvement at day 90 as compared to day 1, Mean heart rate was also reduced at day 90 as compared to day 1, although the difference was not statically significant as shown in table 3.
|
Sr. No. |
Parameter |
Day 1 |
Day 90 |
p-value |
|
1 |
Weight |
66.35+8.22 |
61.68+7.85 |
0.001 |
|
2 |
Abdominal girth |
94.45+6.77 |
88.20+6.69 |
0.001 |
|
3 |
Heart rate |
80.15+11.04 |
76.02+9.19 |
0.08 |
|
4 |
HbA1c |
9.05+1.81 |
7.05+1.06 |
0.001 |
|
5 |
BMI |
26.08+2.94 |
24.29+2.83 |
0.001 |
|
6 |
SBP |
131.18+16.67 |
122.08+15.43 |
0.01 |
|
7 |
DBP |
80.5+9.50 |
73.73+8.18 |
0.001 |
Table 3: Changes in mean values of various parameters at day 1 and day 90 in the patients of present study.
Mean Dukes treadmill score at day 1 was -1.76, whereas day 90 mean reading of Dukes treadmill score was found to be 6.34 and this difference was highly statically significant (Figure 1).
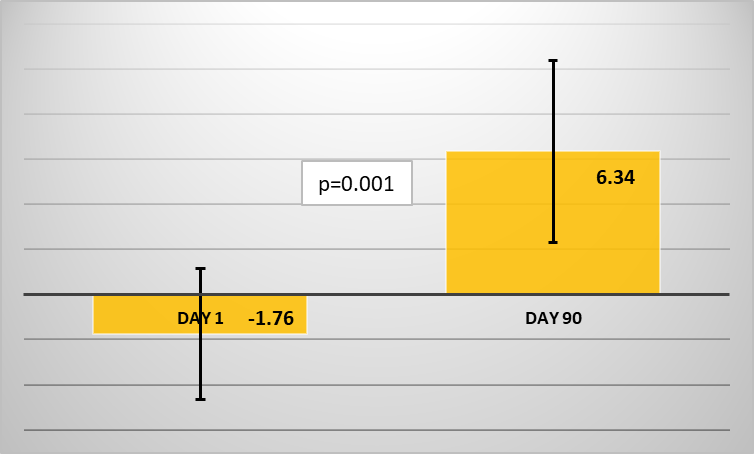
Figure 1: Mean Dukes treadmill score at day 1 and day 90 in patients of present study.
90% of the patients had stopped taking calcium channel blockers, while 84%, 100%, 58% and 100% of the patients had stopped taking beta blockers, vasodilators, diuretics and nitrates, respectively at day 90 [table 4].
|
Drug class |
Day 1 (n) |
Day 90 (n) |
% of patients who stopped medicines |
|
Calcium channel blockers |
10 |
1 |
-90 |
|
Beta blockers |
19 |
3 |
-84.21 |
|
Vasodilators |
2 |
0 |
-100 |
|
Diuretics |
12 |
5 |
-58.33 |
|
Nitrates |
25 |
0 |
-100 |
Table 4: Percentage of patients showing tapering of allopathic medication towards the end of Ischemia Reversal Program therapy.
Discussion: Despite the wide range of therapeutic options available, IHD continues to be a major cause of morbidity and death worldwide. Therefore, it is urgent that novel therapeutic options be sought for the treatment of IHD. The therapeutic effects of the traditional class of anti-ischemic medications include the correction of the imbalance between the heart's oxygen demand and supply, lowering of blood pressure, decreasing platelet activation, hypolipidemic action, antioxidant impact, etc. Similar properties have also been discovered in a number of herbal medicines, offering Ayurveda a formidable and practical alternative to conventional therapy in the treatment of IHD. Ayurvedic doctors provide Panchakarma as an adjunct treatment for the management of IHD.2
The IRP process consists of three steps: Snehana, Swedana, and Basti. The Snehana/ centripetal oleation therapy-anxiolytic effect of IRP is thought to diminish sympathetic overactivity which might help in reducing myocardial workload and oxygen demand. Swedana/ thermal vasodilation in thought to lower salt and fluid levels, which lowers resting preload and may assist in lowering myocardial oxygen demand. For the release of nitric oxide from the endothelium, a decoction of Tribulus terristris, curcumin, and phyllanthrus embelica may be useful. It may also have anti-inflammatory and antioxidant properties. By generating coronary vasodilation, this effect may be beneficial in enhancing coronary circulation.7 In our analysis of the effectiveness of IRP in IHD, we discovered that at 90 days from the start of the entire process, there was a highly significant improvement in Duke's treadmill score, DBP, and SBP.
One predictive indicator for IHD patients is SBP. Since lower SBP lessens the afterload on the ventricles and enhances endothelial function, it is linked to a better prognosis in IHD.8 Most notably, we discovered that after 90 days of therapy, IRP significantly decreased patients' reliance on conventional allopathic medicine.
In patients at risk for IHD, Duke's treadmill score is employed as a diagnostic and prognostic assessment. It is more valued for its function in risk categorization. These individuals do not require coronary angiography for additional assessment if their Duke's treadmill score is below 5, which indicates little risk for cardiovascular complications. Their four-year survival rate is quite close to 100%. Duke's score of -11 indicates a high-risk category, and individuals in this group require coronary angiography for additional assessment. 79 percent of them survive after four years. Scores between -4 and -10 indicate an intermediate risk category. Depending on the patient's condition, these individuals need either a myocardial perfusion scan or a coronary angiography for assessment.6 DTS considerably improved in our study. According to studies, people with IHD who improve their Duke's score and VO2max have a better prognosis.9,10 Therefore, a favorable prognosis is shown by the fact that Duke's treadmill score significantly improved following IRP in our research.
The substantial reliance of IHD patients on traditional allopathic treatment in economically struggling nations like India drives up healthcare costs significantly. Additionally, when these treatments' side effects grow, patients are less likely to take them, which makes the situation even worse.11 In light of this, we examined changes in patients' reliance on allopathic medicine using IRP. At the conclusion of 90 days, there was a noticeable decrease in dependence on practically every type of anti-ischemic medications, along with an increase in the number of patients who stopped taking allopathic medications.
Conclusion: After IRP, there was a noticeable improvement in VO2max, Duke's treadmill score, SBP, and DBP. The patient's dependence on allopathic drugs was significantly decreased. Therefore, IRP may be a strong and practical alternative to the usual allopathic therapy of IHD.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org