
Frederick Chua, MD1; Kenny Vongbunyong, MD1; Deniz Akay Urgun, MD2; Roxana Ghashghaei, MD3
1Department of Medicine, University of California, Irvine
2Department of Radiology, University of California, Irvine
3Department of Medicine, Division of Cardiology, University of California, Irvine
*Corresponding Author: Frederick Chua, Department of Medicine, University of California, Irvine.
Received date: September 20, 2022
Accepted date: September 26, 2022
published date: October 03, 2022
Citation: Chua F, Vongbunyong K, Deniz A Urgun, Ghashghaei R. (2022) “Anomalous Origin of Left Main Coronary Artery from the Right Sinus of Valsalva.” J Clinical Cardiology Interventions, 2(5); DOI: http;//doi.org/04.2022/1.1027
Copyright: © 2022 Frederick Chua. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Anomalous coronary arteries are rare congenital variations with cases ranging from asymptomatic to life-threatening. Given the wide variability of coronary anomalies, it is challenging to predict their clinical consequences. Here, we present the ‘malignant’ variant – inter-arterial course of the left coronary artery – given the high risk of SCD.
Case Description:
A 22-year-old Caucasian man with no prior cardiac history, presented to the emergency department after a syncopal episode while driving a motor vehicle. A full trauma workup was performed including a Computed Tomography (CT) of the chest. The patient was found to have an anomalous origin of the left main coronary artery (LMCA) that originates from a common ostium with the right coronary artery (RCA) at the superior aspect of the Right Sinus of Valsalva (RSV) (figure 1 and 2). There is evidence of inter-arterial course of the LMCA between the aorta and pulmonary trunk (figure 3a and 3b). Cardiothoracic surgery was subsequently consulted. Given how quickly the LMCA dove deep into the septum without an intramural course, surgical unroofing was not performed. Cardiothoracic surgery opted for coronary artery bypass grafting (CABG) with a left internal mammary artery (LIMA) to left anterior descending (LAD) artery anastomosis instead. The patient tolerated the procedure well without any complications and was discharged in stable condition.
Discussion:
Among the different variations of congenital coronary artery anomalies, one of the most critical variants features the LMCA originating from the RSV. There are four further sub-types in which LMCA originating from the RSV can be classified as. These include the following: [1] the LMCA passes between the aorta and pulmonary trunk (inter-arterial), [2] the LMCA passes anterior to the right ventricular outflow tract (prepulmonic), [3] the LMCA courses along the crista supraventricularis in the myocardium or subendocardium and surfaces in the proximal interventricular sulcus (transspetal / intraseptal / subpulmonic), and [4] the LMCA arises to the right of the RCA and circles around posteriorly to the aortic root (retroaortic) [1]. Furthermore, when the LMCA originates from the RSV, the LMCA and the RCA can originate separately or share a common ostium.
Anomalous origin of the left coronary artery from the RSV is rare with an estimated prevalence of 0.02-0.05%2. However, second to hypertrophic cardiomyopathy, it remains a leading cause of cardiac death in young athletes. Most patients are asymptomatic and/or the first manifestation of their disease could unfortunately be sudden cardiac death (SCD). Even in those who are symptomatic, they may experience nonspecific symptoms such as palpitations, syncope, and dyspnea on exertion3.
Multiple hypotheses have been proposed to explain the ‘malignant’ inter-arterial course. This includes [1] the acute angle of the artery’s “slit-like” ostium which results in narrowing of the vessel and decrease in blood flow, [2] a possible intramural aortic segment leading to endothelial dysfunction and coronary vasospasm, and [3] the inter-arterial course which is prone to extrinsic compression of the vessel between the aorta and pulmonary trunk. These mechanisms all contribute to myocardial ischemia when a patient exerts themselves, which may result in fatal arrhythmias and SCD [4]. In this patient case, CT imaging demonstrated both a ‘malignant’ inter-arterial course of the LMCA between the pulmonic trunk and aorta, as well as deep septal course of the LMCA within the left ventricle’s wall (figure 4a and 4b). Therefore, this patient’s specific LMCA course was concerning both extrinsic compression of the LMCA between the aorta and pulmonary trunk and compression of the LMCA from within the left ventricle septal wall during systolic contraction.
Additionally, it is important to note that cardiac CT imaging is typically obtained during diastole. This allows for reduced motion at the time of image acquisition and the opportunity to better visualize coronary arteries as they receive blood flow during diastole in the cardiac cycle. Therefore, cardiac CT images can underrepresent the degree of stenosis coronary vessels experience during systole. Similarly, figure 3b may underestimate the degree of compression experienced by the LMCA, as the image was captured during diastole and not systole when the left ventricle is contracting.
Due to the high risk of SCD with the inter-arterial course, there are consensus guidelines from American College of Cardiology (ACC) and American Heart Association (AHA) which recommend surgical intervention even in asymptomatic patients (Class I, Level of Evidence B). In contrast, other variants of anomalous origin of left coronary artery from RSV are considered benign. Patients with benign variants may not be referred for surgery and do not have exercise restrictions. Multiple surgical approaches have been proposed: [1] surgical unroofing for patients with significant intramural length of the anomalous vessel, [2] reimplantation (ostial translocation) when there is little or no intramural segment, and [3] coronary artery bypass graft with mammary artery or saphenous artery conduit when above approaches are technically infeasible [5].
Conclusions:
Anomalous origin of left coronary artery is rare, but it is one of the leading causes of SCD in young adults. The inter-arterial course is the ‘malignant’ variant due to the highest risk of SCD. Multiple proposed mechanisms contribute to ischemia, including the acute angle take-off, possible intramural segment leading to endothelial dysfunction, and external compression of the vessel by the aorta and pulmonary trunk. Therefore, even asymptomatic patients with this variant may be referred for surgery. Surgical options include surgical unroofing of the intramural segment, coronary reimplantation, and coronary artery bypass graft.
Images:
Figure 1: Rendered 3D Computed Tomography showing course of LMCA
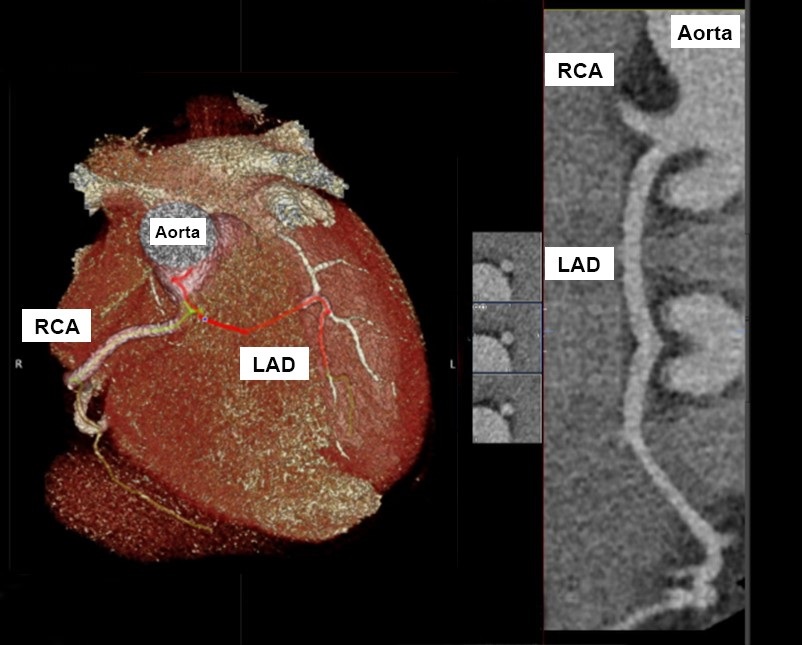
Figure 2: Generated 3D plane of heart
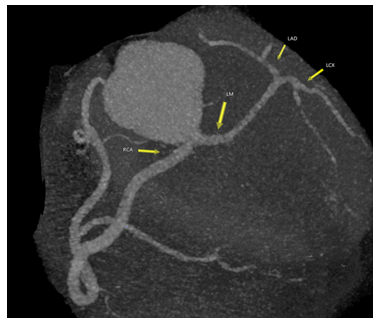
Figure 3a: Computed Tomography Axial view showing common origin of RCA and LMCA.
Figure 3b: Computed Tomography Axial view showing sub-pulmonic and “malignant” course of LMCA (*).
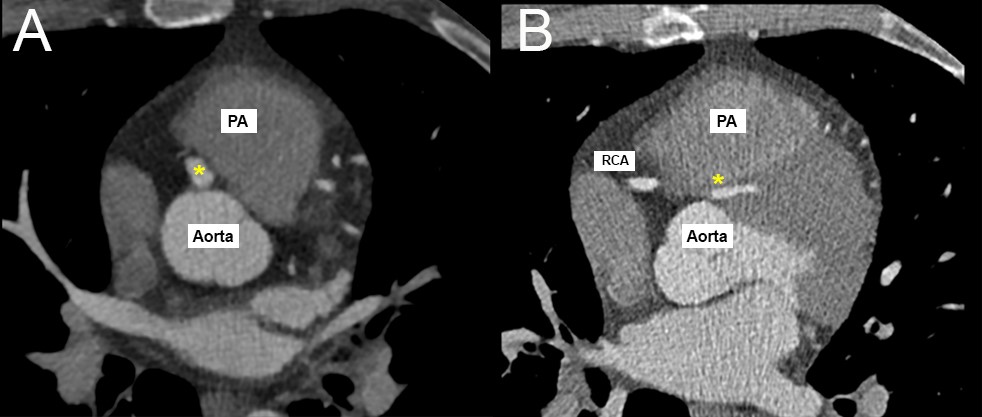
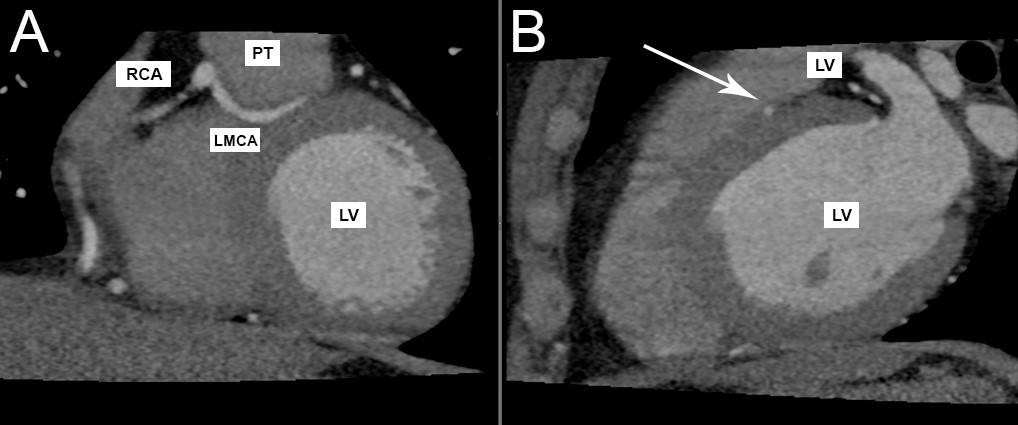
Figure 4a: Computed Tomography Coronal view demonstrating the common origin of RCA and LMCA with the sub-pulmonic course of LMCA.
Figure 4b: Computed Tomography Sagittal view showing the deep septal course of LMCA (arrow) withing LV wall.
Acknowledgments: Not applicable
Funding: The authors declare there is no funding to report.
Conflicts of Interest: The authors declare there are no conflicts of interest to report.
Learning Objectives:

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org