Clinical Cardiology Interventions
OPEN ACCESS | Volume 6 - Issue 1 - 2026
ISSN No: 2836-077X | Journal DOI: 10.61148/2836-077X/JCCI


Rajaram Sharma
Assistant professor, Radio-diagnosis Pacific Institute of Medical Sciences (PIMS), Umarda, Udaipur, Rajasthan, India
Corresponding Author: Rajaram Sharma, Assistant professor, Radio-diagnosis Pacific Institute of Medical Sciences (PIMS), Umarda, Udaipur, Rajasthan, India.
Received date: July 26, 2022
Accepted date: August 03, 2022
published date: August 08, 2022
Citation: Sharma R. (2022) “Revisiting the Role of CT Evaluation in Persistent Truncus Arteriosus.” J Clinical Cardiology Interventions, 2(4); DOI: http;//doi.org/04.2022/1.1024
Copyright: © 2022 Rajaram Sharma. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Truncus arteriosus is a cyanotic congenital heart anomaly in which a single trunk supplies both the pulmonary and systemic circulation, instead of a separate aorta and a pulmonary trunk.It accounts for up to 2% of congenital cardiac anomalies and is almost always associated with a ventricular septal defect (VSD).Patients may present with signs and symptoms of cyanosis or congestive heart failure. Here we present a case came to our radiology department for ultrasonography (USG). Patient had previous antenatal USG report which was normal and was done at 12 weeks of gestational age.
Text:
Persistent truncus arteriosus is a sporadic complex congenital cardiac disease found in approximately 0.7-1.4 % of all congenital cardiac malformations.[1] It is a result of the failure of conotruncal septation during the fetal developmental stage. It has been related to chromosome 22q11 deletion and DiGeorge syndrome. In this anomaly, only one great artery with a single semi-lunar valve originates from the ventricular part of the heart to provide systemic, pulmonary and coronary circulation. The truncal valve is usually more prominent than the normal semi-lunar valve, and its leaflet is thickened and dysplastic. A ventricular septal defect (VSD) is almost always present. There are four types of truncus arteriosus according to Van Praagh&Collettand Edwards's classifications.[2] Type A1 (Collett and Edwards type I), in which a single trunk of pulmonary artery arises from the lateral sides of the truncus, in type A2 (Collett and Edwards type II), pulmonary arteries arise separately from the lateral or posterior aspect of truncus, type A3 has multiple collateralswhich arise from pulmonary arteries and supply the lungs (or pulmonary arteries arising from either side of the trunk independentlyCollett and Edwards type III). In contrast, type A4 truncus is associated with an interrupted aortic arch (Collett and Edwards type IV or pseudo truncus).There are many cardiac and extracardiac anomalies associated with truncusarteriosus like a large membranous ventricular septal defect, coronary arteries anomalies which have 31 % association, pulmonary stenosis (2-10% association), pulmonary artery agenesis and aortic arch anomaly (30-33 %).[3,4] Other rare associations include lung hypoplasia, criss-cross pulmonary arteries, persistent left or double superior vena cava. The standard treatment protocol is early surgical repair which includes VSD patch closure and detachment of the pulmonary arteries from its trunk and restoring its continuity with the right ventricle.
A three-day-old female child was referred to our hospital with a low oxygen saturation level. As per the mother, she didn't undergo any ante-natal ultrasound scan, and the birth history was unremarkable.On physical examination baby weighed 2.6 kg, had tachypnea and was maintaining 60 to 70% oxygen saturation. The chest radiographrevealed cardiomegaly and echocardiography suggested a possible truncus arteriosus physiology. Therefore, Cardiac computed tomography (CT) scan was prescribed to map the exact anatomy of the common arterial trunk and pulmonary vasculature and look for associated anomalies.[5] Cardiac CT revealed a large single arterial trunk overriding the membranous ventricular septal defect without any demonstrable stem of the main pulmonary artery. Right, and left pulmonary arteries were arising separately from ascending aorta above the truncus valve on the same side (left postero-lateral side).[Figure 1,2& Video 1] Right and left pulmonary arteriesweresmaller and measured 4 mm and 3.5mm, respectively.
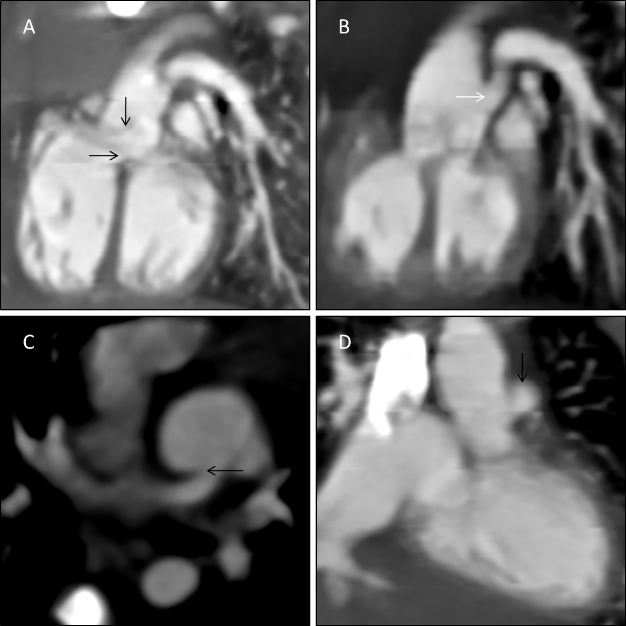
Figure 1: (A,B& C) 3-Dimensional volume rendered technique (VRT) images precisely demonstrate correlation between the abnormal vessels; note that the stem of pulmonary arteries is arising from left lateral side of the common trunk ( black arrow).
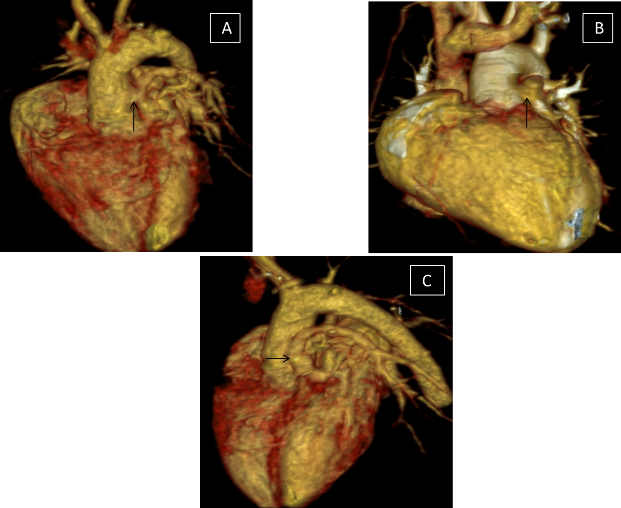
Figure 2: Cardiac CT scan images (A & B) in sagittal plane demonstrate single arterial trunk (truncus) overriding the membranous ventricular septal defect (Black arrows) and the pulmonary arteries arising from ascending common trunk above the truncus valve on left poatero-lateral side (White arrow). (C & D) Axial and coronal planes images respectively, depicting the origin of pulmonary arteries fromtheproximal common trunk (Black arrow).
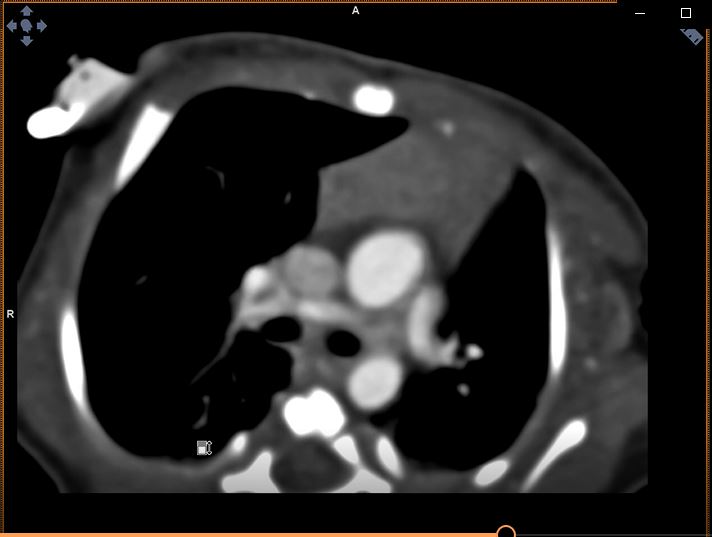
Video Picture 1: Computed Tomography (CT)scan, WMF video format: Axial plane movie clip of thorax shows pulmonary arteries arising from postero-lateral aspect of ascendind aorta and has narrow calibre.
Additionally, both the atria were also dilated. Ascending aorta and descending aorta had standard calibre. Due to all these findings, a persistent truncus arteriosus (Collett and Edwards type II) diagnosis was made.
After the counselling, the parents didn't opt for the surgery and asked for discharge because of an extremely poor prognosis.
Conclusion:














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org