Pediatrics and Child Health Issues
OPEN ACCESS | Volume 6 - Issue 1 - 2026
ISSN No: 2836-2802 | Journal DOI: 10.61148/2836-2802/JPCHI


Gaurav Gupta 1*, Manohar Bhat 2, Abhishek Khairwa 3
1Paediatric and Preventive Dentistry, Professor post at Department of Paediatric and Preventive Dentistry in Jaipur Dental College, Private Practice at Wisdom Dental Clinics, Jaipur, Rajasthan
2Professor and Head post at Department of Paediatric and Preventive Dentistry in Jaipur Dental College Jaipur, Rajasthan
3Professor post at Department of Paediatric and Preventive Dentistry in Jaipur Dental College Jaipur, Rajasthan
*Corresponding Author: Gaurav Gupta. Department of Paediatric and Preventive Dentistry in Jaipur Dental College, Private Practice at Wisdom Dental Clinics, Jaipur, Rajasthan.
Received: January 02, 2023
Accepted: January 24, 2023
Published: February 28, 2023
Citation: Gupta G, Bhat M, Khairwa A. (2023). “Managing Early Childhood Caries with Minimally Invasive Approach: A Case Series”, J Pediatrics and Child Health Issues, 4(1); DOI: http;//doi.org/03.2023/1.1052.
Copyright: © 2023 Gaurav Gupta. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.Abstract: 100 words
Caries can affect early permanent dentition if child has improper dietary habits and poor oral hygiene maintenance. Aim of current study is to present treatment approach in case of severe early childhood caries (ECC) with minimal invasive dentistry to restore and form function of dentition. Therefore, early diagnosis and initiation of preventive and restorative therapies are imperative in its management.
Introduction
Premature loss or severe destruction of primary teeth due to caries is common occurrence in children under 6-years-old, known as Early Childhood Caries (ECC). This by nature is rampant, acute and progressive. If progression of caries condition is not interrupted, serious local, systemic, psychological, aesthetic, and social problems could be resulted.[1]
Restoration of primary teeth destroyed due to caries is challenge for paediatric dentists, due to child behaviour and age. Various aesthetic options are available for restoring or replacing it and it depends on clinician to make best decision for each individual situation. Adhesive restorations, such as direct composite resin veneer, allow clinicians to restore and to create minimally invasive preparations, thereby preserving tooth structure.[2] Minimally invasive operative technique for managing cavitated lesions in young children by restoring tooth with aesthetic crown sealing carious lesion after caries removal and restoration preserves tooth till eruption of succedenous tooth. In more severe cases, when extractions are needed, space should be maintained functionally as well as aesthetically by a suitable space maintainer. This rehabilitation should provide good longevity, without interfering with normal eruption process.[3]
Digital impressions represent innovative methods that enable dentists to construct virtual, computer-generated copy of hard and soft tissues of oral cavity, with use of lasers and other optical scanning machines. Digital method captures impression data with great accuracy, in minutes, without need for traditional impression resources that some patients find inopportune and messy. Patients consider digital impressions to be easier and more comfortable method, in comparison with classical impression techniques. Impression information is then moved to computerized workstation that creates restorations. Once impression is captured, it can be either sent to laboratory/ in house manufacturing unit, or to CAD/CAM application with help of one click, and in second, laboratory or chairside system receives all information needed.[4]
To maintain smooth conversion of infant’s jaws to adult form, nature has given two series of dentition. If there is any deviation, then jaw form and overall facial profile along with psychology of an individual may be altered. Due to caries early loss of maxillary incisors is very common in young children and before two-third of roots of permanent incisors are formed. So, space should be maintained functionally as well as aesthetically by suitable space maintainer depending on dental age of patient. Space maintainer may be of removable, fixed, semi-fixed, functional, or non-functional type.[5]
Current case series describe management of ECC with minimal invasive approach with use of intraoral scanners in making digital impressions for fabrication of chairside crown and in placement of pre- fabricated space maintainer.
Case report
Case 1
An 8-year-old boy came to clinic with decayed tooth and pain in mandibular back region. A medical, as well as clinical history was taken along with the radiographic examination, which showed the presence of deep dentinal caries with pulpal exposure and extensive loss of tooth structure in the right primary mandibular 2nd molar. The tooth was found to be tender on percussion. (Figure1a, b)

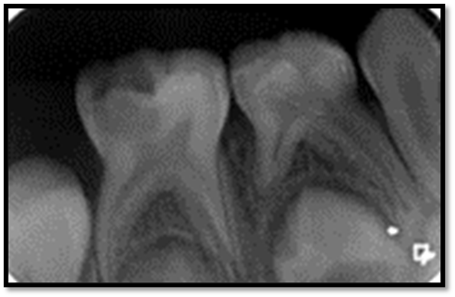
Figure 1a: Intraoral photograph ,1b IOPA of right primary mandibular 2nd molar
The tooth required a full-coverage restoration after endodontic treatment; both the child and the parent were highly concerned with the aesthetic appearance of the restoration. We decided to restore the primary mandibular right second molar with a paediatric zirconia crown using intraoral scanning and chairside milling.
We achieved local anaesthesia with NOIS (Nitrous Oxide Inhalational Sedation). We have modified our protocol here for the procedure exclusively for digital dentistry in paediatric patients; here we directly went on for tooth preparation, thereby utilizing the time taken by local anaesthetic to express its effect. Scanning was done by intraoral scanner (Dentsply Sirona Omnicam) after minimal tooth preparation to capture a digital impression for further processing in CEREC (Chairside Economical Restoration of Aesthetic Ceramics, or Ceramic Reconstruction) software.
A Digital record of the segment with opposing arch was also recorded. Scanning provides easier, more intuitive, and precise 3D models in natural colours in less than 2 minutes. [Figure 2]
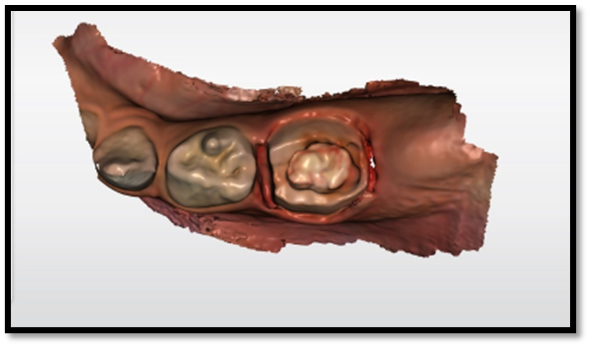
Figure 2: Intraoral scan
After this we perform Pulpectomy procedure meanwhile designing and milling of the restoration was done by supporter staff. [Figure 3 a, b]

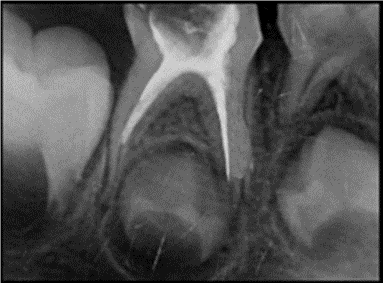
Figure 3 a, b: Intraoral photograph and IOPA after pulpectomy
Designing was done in 5 minutes followed by milling in the primemill which took around 11minutes. [Figure 4a, b, c]
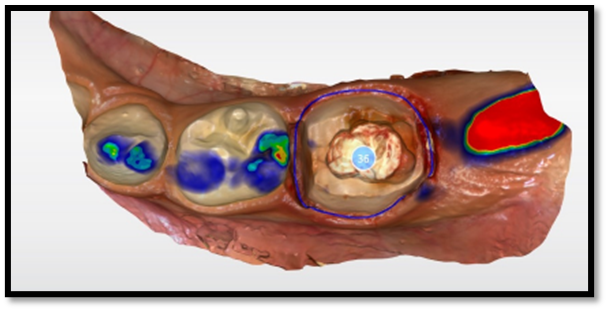
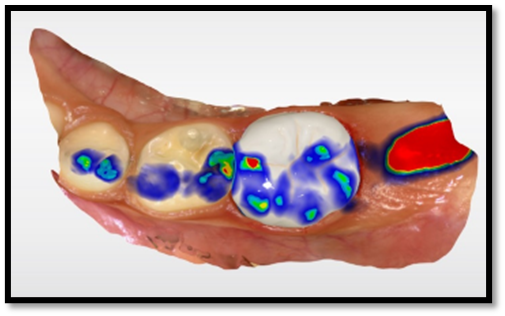
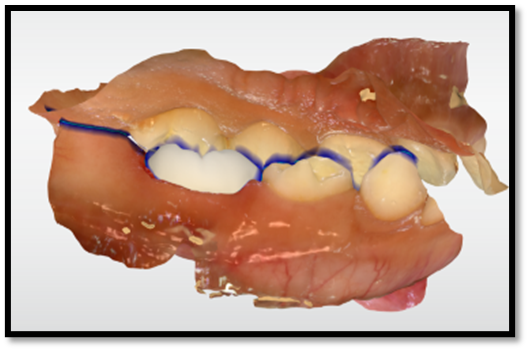
Figure 4 a, b, c: Customized CAD designing
By the time pulpectomy was done we utilise time by preparing zirconia crown with chairside milling. Sintering was done which provide adequate strength and glazing is done prior to cementation which makes surface more plaque resistant. The tooth and the crown were cleaned of all blood residues. Glass ionomer cement (Fuji One PLUS, GC, Louvain, Belgium) was used for the cementation. [Figure 5 a, b]

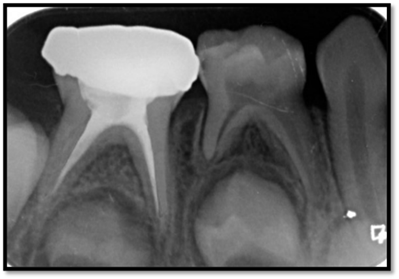
Figure 5 a, b: Cementation done
Excess cement was removed from interdental spaces and group function occlusion was checked. The patient was given post-operative instruction. [Figure 6 a, b]


Figure 6 a, b: Occlusion was checked
In a matter of less than 45 minutes, complacent, enjoyable, and acceptable results were achieved. As shown in this case, we reconstituted not only the form and function but also the aesthetics with minimally invasive dentistry in a single sitting with the help of the CEREC workflow.
CASE 2
A 4.5-year-old boy reported to clinic with a chief complaint of pain in the upper left back teeth region since one week. Clinical examination revealed deep carious lesion with grade 2 mobility in primary maxillary first molar [Figure 1]

Figure 1: Intraoral photo
The associated IOPA radiograph showed decayed in primary maxillary first molar tooth [Figure 2].
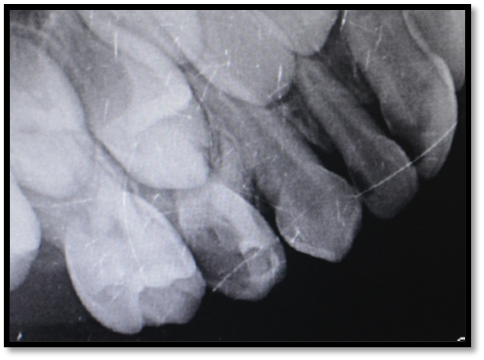
Figure 2: IOPA of affected side
It was decided to extract upper left first deciduous molar as it does not show good prognosis. So to maintain space for eruption of its succedenous tooth space maintainer was planned. Band and loop type of space maintainer was indicated in the present case.
After extraction of decayed tooth under antibiotic coverage [Figure 3], preformed band and loop space maintainer was placed chairside in single sitting in the socket to touch and guide the vertical eruption path of the unerupted permanent maxillary left first molar. Procedure is handy, chairside, economical and has better patient compliance as compared to conventional space maintainers and is minimally invasive [Figure 4,5].

Figure 3: Intraoral photo after extraction

Figure 4: Placement of space maintainer

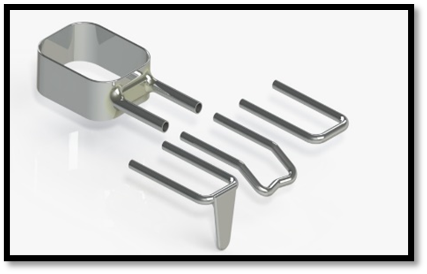
Figure 5: Prefabricated space maintainer
The recall visits were planned after every two months to check the condition of the band and loop space maintainer, supporting teeth and status of eruption of permanent teeth.
The recall after 10 months showed signs of eruption with pre-eruption bulge around it. It was then decided to remove the band and loop and the patient was closely monitored during the recall visits till its succedenous tooth gets erupted.
Discussion
Early childhood caries can be defined as presence of one or more carious lesions, cavitated or not, in children up to five years of age [2,3]. It represents result of an imbalance between multiple risk factors and protective factors that leads to pain, early dental loss, malnutrition, growth retardation, difficulty in chewing, speech problems, general health disorders and psychological problems. ECC also contributes to loss of self-esteem and future damage to permanent dentition [6,7,8,9]
Through anamnesis and dietary diary of patient reported, a low-nutrient and high-frequency diet was observed regarding intake of sugary foods and beverages, especially at night. The literature confirms that dietary practices are an important cause of ECC, specifically through consumption of sugary drinks and a diet rich in sugars and starches [7,10]
Use of aesthetic restoration has become an important aspect of paediatric dentistry. This case report describes single-visit fabrication of zirconia crown on a primary molar. To limit chairside time and promote quality of care given, CAD/CAM technology could be used in cases when a crown on primary tooth is needed. With the help of the digital design software, clinician can provide better minimally invasively marginal fit crowns without traditional impression procedures in non-competent child patients.
Complete digital workflow through chairside systems allows indirect restorations to be carried out in same clinical session in which preparations are made. This prevents temporization, inflammation of tissues, greater comfort for patient and a rapid workflow for dentist [11]. We also placed crown through CEREC workflow in same visit without conventional impression method.
This in comparison with procedures where several sessions were performed, and laboratory work required more time between session and session [12]. Quality of adjustment of restorations made through CAD-CAM systems is equal to or better than restorations performed conventionally both in clinic [13] and in a laboratory using indirect techniques on physical models obtaining clinically acceptable results [14].
Teeth may be lost due to trauma, ectopic eruption, congenital disorders, premature resorption due to arch length deficiency and further more; dental. Early loss of the primary molars had a significant effect on dental arch length and resulted in 2–4 mm of space closure per quadrant in both arches. The most considerable space loss had been attributed to mesial movement of the permanent molars. Bands and loops are being has been used since long as space maintainer with good high success rates Baroni et al., [15] Rajab [16]; Fathian et al., [17] in spite of good patient compliance, disintegration of cement, solder failure, caries formation along margins of band and long construction time are some of disadvantages associated with them.
The fixed space maintainer is indicated to preserve dental arch integrity. In our second case we placed preformed band and loop space maintainer chairside only which was minimally invasive and quick, no impression was needed. [18]
These methods reduce chair side time in paediatric patient and minimally invasive approach; with enhancements in patient compliance and comfort, thus switching to digital procedures may have positive impact on paediatric patient’s perception of dental procedures thereby eliminating the need of alginate impression
Conclusion
The ceramic materials and CAD/CAM technologies are increasingly being used in aesthetic dentistry for both adults and children. There are many evidences in the literature for CAD/CAM technology usage in primary and permanent dentition in childhood age. This gives the possibility to restore children’s dentition with contemporary metal-free ceramic constructions, providing better adhesive, aesthetic and functional restorations in single sitting. Dental space maintenance is essential in cases of premature loss of primary dentition to prevent malposition, supra-eruption, or crowding of the developing permanent teeth. Various types of space maintainers are available and each type is specifically designated for indications. The goal is to develop a perfect and healthy occlusion in permanent dentition by timely management of cases with ECC with minimal invasive approach.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org