
Nagaveni NB
Consultant Pediatric Dentist, Dental wing, Karnataka ENT Hospital and Research Centre, Chitradurga, Karnataka, India.
Corresponding author: Nagaveni NB, Consultant Pediatric Dentist “Garike Dental Care’ Davangere, Karnataka, India.
Received Date: July 06, 2024
Accepted Date: July 14, 2024
Published Date: July 26, 2024
Citation: Nagaveni NB, (2024). “Dental malformations and anomalies in a cleft lip and palate patient”. Pediatrics and Child Health Issues, 4(1); DOI: 10.61148/2836-2802/JPCHI/061
Copyright: © (2024). Nagaveni NB, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cleft lip and palate is a major congenital orofacial deformity affected the whole family including parents, patient and guardians. This facial deformity is associated with various problems requiring broad range of treatment at every stage of child development from birth to adolescence. Various dental malformations and anomalies or conditions are encountered in children with cleft lip and palate necessitating appropriate treatment. The present article demonstrates occurrence of different dental anomalies in a pediatric patient affected with cleft lip/palate thereby high lightening an awareness about these conditions among health professionals dealing with children to provide a holistic care.
cleft lip and palate; dental malformation; supernumerary tooth; supplemental incisor; tooth anomalies
Dear Editor-In-Chief:
An 11-year-old female patient reported to a private dental clinic complaining of malformed tooth in the upper front region of the oral cavity. Patient was a known case of cleft lip and palate deformity and has been taken treatment for the cleft lip. Patient was moderately built and nourished with good behaviour. Intraoral examination showed presence of cleft palate and alveolus in the maxillary anterior region which was still not treated. A mixed dentition consisting both primary and permanent dentition was observed. In the maxillary arch, left central incisor appeared malformed having defective crown structure. The permanent right lateral incisor appeared smaller in size compared to left lateral incisor. Patient was subjected to a panoramic radiographic examination to study in detail about all dental components. Examination of the radiograph showed presence of a tooth resembling lateral incisor. This extra tooth was impacted in mesio-angular position (Figure 1). Both crown and root appeared normal in structure and found similar to the lateral incisor. The erupted lateral incisor was smaller in shape with short root having moderate dilaceration at the apical portion (20-degree-bend). The crown of the central incisor had defective enamel formation. But its root component was normal in appearance and structure (Figure 1). Both erupted and impacted lateral incisors were located at the cleft region. No other dental findings were observed. Based on radiographic features the case was diagnosed as cleft palate associated with dysmorphic central incisor and supplemental lateral incisor. Patient details are described in Table 1. Patient was scheduled for comprehensive treatment including both dental and surgical aspect.
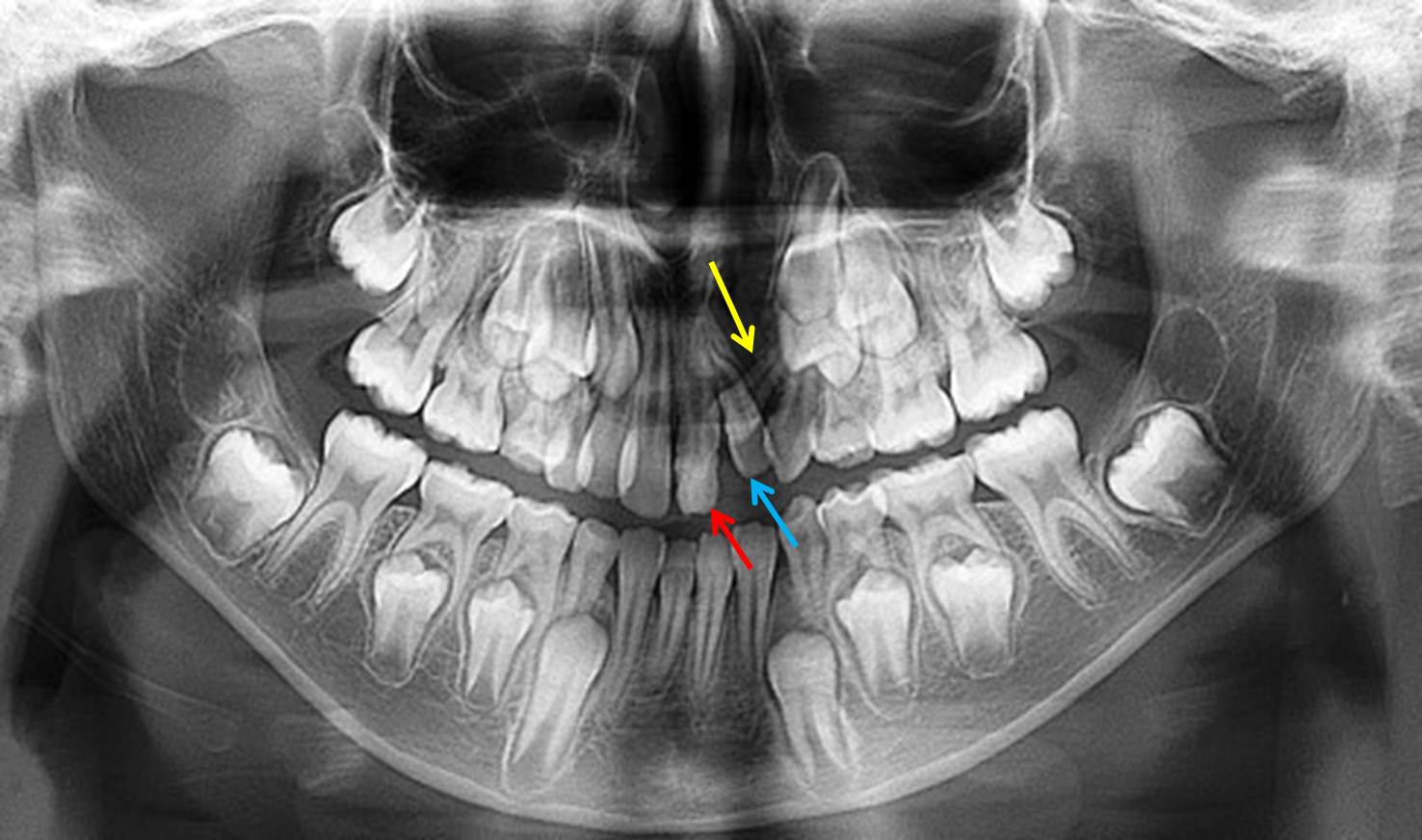
Figure 1: Orthopantomograph radiograph showing dysmorphic permanent maxillary left central incisor (red arrow). Permanent lateral incisor (blue arrow) and an impacted supplemental supernumerary lateral incisor (yellow arrow) in the cleft region are also present.
|
Age & Gender |
Chief Complaint |
Clinical Features |
Status of Cleft Lip/Palate Unilateral/Bilateral |
Dental Anomalies/Malformations observed |
|
11 years Female |
Presence of a malformed tooth in the upper front region |
Dysmorphic permanent maxillary left central incisor |
Unilateral |
Impacted supernumerary supplemental maxillary left lateral incisor Permanent maxillary left lateral incisor with root dilaceration Dysmorphic permanent maxillary left central incisor |
Table 1: Demographic details of the presented case with cleft lip and palate
Cleft lip and palate/alveolus are the commonly seen orofacial congenital malformation in neonates. These children require meticulous presurgical treatment therapies for their survival before initiation of definite surgical therapy. This orofacial defect not only affects the neonate but also the whole family get disturbed psychologically, emotionally and financially. Apart from natal and neonatal teeth seen in these infants, various other dental anomalies or deformities are also encountered [1-3]. When the neonate found with a cleft lip or palate defect the foremost treatment strategy required is the presurgical naso-alveolar moulding in order to mold the cleft alveolus and finally to obtain best post-surgical results following definitive primary and secondary surgeries. However, there is lack of knowledge and awareness about this new treatment approach among care takers and health professionals [4]. A recent bibliometric analysis demonstrated the lack of major contribution from many countries about naso-alveolar molding therapy strongly indicating further research in this domain [5-7].
Lasota in 2021 [8] reviewed the literature about the occurrence of dental anomalies in cleft lip with or without palate. The most dental anomaly found was the teeth agenesis with a prevalence of 28% to 66% in these patients. Permanent dentition was more affected (52.7%) compared to primary dentition (16%). At the cleft side, lateral incisor was most often found to be missing. Hypodontia increased with severity of the cleft defect. Evaluation of supernumeraries resulted in 17% of the primary dentition and 5.7% for the permanent maxillary dentition. Maxillary lateral incisor is the most commonly found supernumerary tooth both inside and outside the cleft and exhibited different variations in morphology and size. Author reported that anterior maxilla is the main area found with supernumeraries’ teeth. Lateral incisor in the cleft area more often appeared peg shaped with microdontic and sometimes found with enamel hypoplasia in 8.9% of cases. Taurodontism was observed in 15% of cases and macrodontia was found in 12% cases. Other dental abnormalities like canine impaction were also observed in the range from 0 to 58% in comparison with other cleft centres studies. In the cleft area, rotations of central incisors were found in 86% cases followed by transposition of maxillary canine and first premolars in 5% of cases. In the present case, dysmorphic crown was observed in the maxillary permanent left central incisor. All primary teeth appeared normal. An impacted supernumerary supplemental lateral incisor was observed in the cleft area whereas its normal permanent counterpart was clinically erupted and rotated. Moderate degree of root dilaceration (20-degree-bend) was observed in the permanent maxillary left lateral incisor.
With respect to cleft severity the three most common dental anomalies observed are supernumerary teeth, congenital agenesis of maxillary lateral incisors and mandibular incisors. The maxillary lateral incisor is the most frequently affected tooth in the cleft area. Dental anomalies in cleft patients are more commonly reported in males than females. But in the present case, it was found in female patient. In case of complete cleft lip or palate, supernumerary teeth are typically situated distal to the cleft. In the case described here, the same finding was observed consisting of supernumerary supplemental permanent maxillary lateral incisor which was impacted. However, all primary teeth were found normal. In addition to this the permanent central incisor found dysmorphic. Therefore, the present case presentation strongly demands for necessity of experienced specialists including multidisciplinary team work to provide utmost overall care for these children affected with cleft lip/palate.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org