Pediatrics and Child Health Issues
OPEN ACCESS | Volume 6 - Issue 1 - 2026
ISSN No: 2836-2802 | Journal DOI: 10.61148/2836-2802/JPCHI


Sunil Malik1*, Kanika Yadav2, Ajay Punj3
1Associate Professor, Department of Pediatrics, Subharti Medical College, Meerut.
2Junior Resident, Department of Pediatrics, Subharti Medical College, Meerut.
3Professor, Department of Pediatrics, Subharti Medical College, Meerut.
*Corresponding Author: Sunil Malik, Associate Professor, Department of Pediatrics, Subharti Medical College, Meerut, UP- 250005, India..
Received Date: March 21, 2022
Accepted Date: April 28, 2022
Published Date: May 04, 2022
Citation: Sunil Malik, Kanika Yadav, Ajay Punj (2022). “Common Psychosocial Health Problems among Adolescent Girls in Northern India”, J Pediatrics and Child Health Issues, 3(3); DOI: http;//doi.org/03.2022/1.1044.
Copyright: © 2022 Sunil Malik. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
Background: About 21% (243 million) of Indian population is adolescents. The psychosocial health status of an adolescent affects their health status in adulthood.
Objective: To assess the prevalence of common psychosocial health status in school going adolescent girls of Northern India.
Methods: A cross sectional study conducted over two years (2018-2020), by the Department of Pediatrics at tertiary healthcare centre. One thousands adolescent (10-19 years) girls from twelve schools (both government and private) situated in nearby districts around 25km from hospital were included. Self-administered structured questionnaire was used for data collection from each participant. The questionnaire included questions on depression was assessed by using Hamilton scale of depression and anxious behaviour was assessed using Hamilton scale of anxiety, shuttering and substance (tobacco/alcohol) abuse.
Results: The study comprised of 1000 adolescents (aged 10-19 years) school girls, of which 37.1%, 25.5% and 37.4% of the subjects belonged to 10-14, 15-17 and 18-19 year of age group respectively. Majority of the girls were from Hindu religion (80.3%). The majority of girls were studying in private school (67.6%) and 32.4% of total girls in government school. Anxiety prevalence was 1.2% and 5.2% of total girls were found in depressed mood. Stuttering was reported among 0.9% of the girls. Prevalence of smoking alcohol and substance abuse in our study was nil.
Conclusion: To achieve wholesome adolescent health, a multidimensional approach with special emphasis on mental health, behaviour change towards healthy lifestyle is required. Mass Screening of adolescent is required to tackle psychosocial problems.
Introduction
According to WHO, Adolescents are the young people aged between 10 to 19 years. About 21% of Indian population is adolescents (about 243 million) [1]. They are the future of the nation, forming a major demographic and economic force. The term “psychosocial” refers to the interplay between the biological, physiological, emotional, cognitive, social, and environmental and the maturational factors. Each of these factors should be considered when the problems and the needs of the adolescents are evaluated [2]. Psychological changes occur largely because the way adolescents see themselves changes dramatically.
Adolescents are a group of apparently healthy individuals. The psychosocial health status of an adolescent determines the health status in his/her adulthood. Many serious diseases in adulthood have their roots in adolescence.
This is particularly among adolescent girls especially in rural India, who also face gender discrimination considering deep rooted culture of patriarchy and hierarchy which trap and modulate their growing socialization. In Indian culture setup adolescent girls by and large emulates cultural and family values prescribed by the religion, caste and ethnic group of their identity, and their personal, vocational and even reproductive choices are based on conservative traditional values as a norm with a few exceptions. Further, the adolescent populations, especially girls have important bearing on the expected demographic, social and psychological makeup and profile of the country [3].
Anxiety disorders are a group of mental health disorders, characterized by excessive feelings of anxiety and fear, the anxiety being worry about future events and fear, a reaction to current events causing physical symptoms such as a racing heart and shakiness. Fear and anxiety are in the same continuum, fear is the reaction to a present danger, an adaptive and evolutionary refined process, and anxiety is the response to a potential threat. Anxiety is a disproportionately intense, chronic and potentially irreversible reaction to an imagined threat, operated through brain-body-emotion- cognitive-changes and their interaction with the environment [4-6].
Historically, children were not considered candidates for depression. Today, childhood depression is widely recognized, and health professionals see depression as a serious condition affecting both adolescents and young.
Although adolescence comprises of one decade of a life span, it is a prelude to the ultimate life that the individual will be destined to live. Thus, those who are going through this period of life require special attention from the family, community and the society as a whole.
Aims & Objectives
The prime objective of this study was to assess the prevalence of psychosocial health status among school going adolescent (aged 10-19 years) girls of Northern India.
Materials and Methods
This was a cross sectional study which was conducted over the duration of two year (2018-2020), in the Department of Pediatrics at Tertiary healthcare centre.
A total of 12 schools, both government and private in nearby districts around 25km from hospital were included in the study. The sample size was calculated by using formula: n= {(Zα\2)2pq}/L2, where n = desired sample size, Zα\2 = standard normal deviate (taken as 1.96 for confidence level of 95%), p = proportion in the target population estimated to have a particular characteristic (prevalence in percentage), q = 100-p, L = allowable error (5% p). So, to calculate prevalence taken was 9% as per States Census 2011 and least allowable error was taken (5%). The required sample size thus calculated was 124. But in our study we have included 1000 school going girls of rural western Uttar Pradesh to get more reliability and accuracy in our results.
The inclusion criteria were adolescent (age 10-19 years) school going girls, present on the day of the study visit and agreed to participate in the study.
The questionnaire performa used in this study was developed indigenously, taking consideration of rural setup and appropriate to adolescent girls. The questionnaire included questions on mental health, substance (tobacco/alcohol) abuse and shuttering. Depression was assessed using Hamilton scale of depression (HAM-D) [7] and anxious behaviour was assessed using Hamilton scale of anxiety (HAM-A) [8].
The obtained data were collected and analyzed. Statistical analysis was done using SPSS software. Difference between two groups was determined using chi square test and the level of significance was set at p < 0.05.
Results
Demographic
The study comprised of 1000 adolescents (aged 10-19 years) school girls, of which 37.1%, 25.5% and 37.4% of the subjects belonged to 10-14, 15-17 and 18-19 year of age group respectively. Majority of the girls were from Hindu religion (80.3%). The majority of girls were studying in private school (67.6%) and 32.4% of total girls in government school.
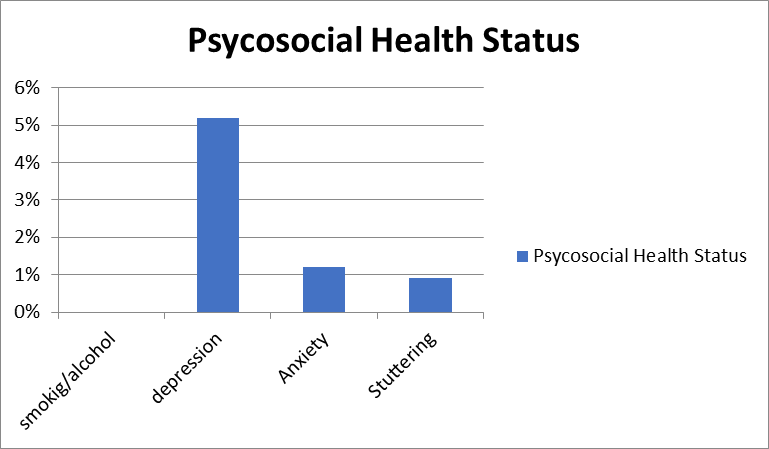
Psychosocial health status
Prevalence of smoking alcohol and substance abuse in our study was nil. Depression was assessed by using Hamilton scale of depression, 5.2% of total girls were found in depressed mood which was statistically insignificant (p value-0.9) (Table.1). Anxious behaviour was assessed using Hamilton scale of anxiety. Anxiety prevalence was 1.2% among girls, statistically insignificant (p value-0.31). Stuttering was reported among 0.9%, of the girls (Figure.1).
|
S.No. |
Parameter |
Mean |
P-value |
|
1 |
Smoking/ Alcohol/ Substance abuse |
Nil |
- |
|
2 |
Depression |
5.2% |
0.9 |
|
3 |
Anxiety |
1.2% |
0.31 |
|
4 |
Stuttering |
0.9% |
- |
Table 1: Psychosocial health status
Figure.1
Discussion
In developing country like India due to poverty and prevailing socio-cultural milieu a substantial number of school children from pediatric age to adolescents suffer from various diseases which can be prevented if diagnosed and treated early and preventive measures taken in time.
School health screening is an important aspect of any community health programme. It consists of tools applied to healthy pupils to detect those with particular health problem that require further evaluation by a specialist. There are many health problems among school children in developing countries like India. Little attention is paid to this important issue.
School health screening provides a unique opportunity to positively impact the health of students-
It acts as a safety net for children who might not have regular access to primary care
Prevent medical, psychosocial, and academic consequences of missed diagnoses
Provide an additional point of contact to develop rapport, educate, and evaluate the overall well-being of students.
In our study, depressed mood was found among 5.2% of the girls. In a study by Aradhya GH et al [9], the prevalence of depression was 2%, which is lower than our study. In a study which was done at Thiruvananthapuram, India, the prevalence of depression was 2.6% [10].
Substance abuse is yet another serious issue as adolescents are ignorant about its consequences. NFHS–3 data shows, in the age group 15–19, 1% of adolescent girls had consumed alcohol. About 4% girls use some kind of tobacco. The average age at tobacco use initiation was earliest at 12.3 years and alcohol usage at 13.6 years among adolescents [11]. In our study, smoking, alcohol and substance abuse was found nil among girls. This may be due to underreporting by girls during study which may be due to social pressure. A study done in Chennai [12] reported that parental substance abuse and lack of parental supervision leads to adolescent substance abuse.
Anxiety was reported in 1.2% of total girls in study. Similar prevalence of anxiety was revealed by Aradhya GH et al [9] in their study (1%). In a study which was done on school going adolescent girls in Delhi, it was found that the most common problem was anxiety/depression, which accounted for almost 10% of all the problems which were faced by adolescents.
In our study, stuttering was found among 0.9% of the subjects. Stuttering was seen in 1% of the girls as reported by Aradhya GH et al9. In a similar study which was done in urban Delhi, the prevalence of stuttering was high i.e. 5.3%.
In our study, mental and physical harassment were nil. Sexual abuse is one of major problems faced by adolescent girls and boys equally. These problems mostly go unnoticed as the victim suffers in silence because of fear and social stigma. This indirectly affects the physical health, mental health and the academic performance. In a study by Kelly Rose-Clarke et al [13] conducted in eastern India, 18% of girls aged 10–14 years had been exposed to emotional violence and 0.3% to sexual violence. Among older girls, 9% had experienced physical violence and 1% sexual violence.
Conclusion:
Promoting and protecting adolescent health will lead to great public health, economic and demographic benefits. Adolescent friendly clinics need to be widely established throughout India and should achieve universal coverage will help set a pattern of healthy lifestyles and reduce morbidity, disability and premature mortality later in adulthood.
Mass Screening in schools or Community based survey of adolescent on regular basis could be an effective tool to control the existing disease and to update occurrence of any new diseases. “Adolescent girls” further need special consideration because of gender inequality and illiteracy especially in rural area. Offering such opportunities to the growing children gives them a chance to build a safe, happy, healthy and productive nation in the future. Adolescent girl’s psychosocial health should be at utmost care as it will help in making women more independent, and also contribute in rising of economy of country.
Various programmes launched by government needs to be reinforced and more awareness to be created among people about these programmes.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org