Neurosurgery and Neurology Research
OPEN ACCESS | Volume 7 - Issue 1 - 2025
ISSN No: 2836-2829 | Journal DOI: 10.61148/2836-2829/NNR


Umi Budi Rahayu1*, Wahida Ratnawati2, David Blow3
1Department of Physical therapy, Faculty of Health Science, Universitas Muhammadiyah Surakarta, Indonesia. 2RSUD Tenriawaru Bone, Sulawesi Selatan; Universitas Hasanuddin Makassar, Indonesia.
3NeuroMuscular Taping Institute, Italy.
*Corresponding Author: Umi Budi Rahayu. Department of Physical therapy, Faculty of Health Science, Universitas Muhammadiyah Surakarta, Indonesia.
Received date : December 14, 2021
Accepted date : November 20, 2021
published date : January 06, 2022
Citation: Umi B Rahayu, Ratnawati W, Blow D. “NeuroMuscular Taping (NMT) Application on Bell’s Palsy: A Case Report”. J Neurosurgery and Neurology Research, 3(1); DOI: http;//doi.org/011.2022/1.1034.
Copyright: © 2022 Umi Budi Rahayu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This case report demonstrates a NeuroMuscular Taping (NMT) application as physiotherapy treatment for bell’s palsy and reports its results. An 18-year-old student with complaints pain in her left lateral neck and ear, decrease left facial muscle strength and facial expression problem. She received a treatment program, which consisted of NMT application, exercise activation, and education home program. The program was performed for 30 minutes per session, twice a day, for 4 times treatment. Before the intervention, the patient really feels discomfort in the area around the left ear and neck, face drop and loss of movement the face on the left side. After treatment, the pain in the area around ear and neck on left side was reduced from 8/10 to 2/10 after first treatment using numerical rating scale, and symmetrical face were remarkably improved using the Ugo Fisch Scale measurement. Moreover, NMT application has been shown to provide a faster for normalization function of the face. Our results suggest that a designed NMT application, exercise, and education home program on the neck and face may be beneficial in the face symmetrical and functional recovery as well as make be comfortable on the area around ear and neck from bell’s palsy.
Introduction
Bell’s palsy is a form of peripheral facial palsy with sudden onset over 24–48 h, involving the superior and inferior areas of the hemiface and affecting voluntary, autonomic and emotional. It may be preceded by uricular or retro-auricular pain, hyperacusis and/or facial paresis palsy (Fieux et al., 2020). Bell’s palsy is a rapid unilateral facial nerve paresis (weakness) or paralysis (complete loss of movement) of unknown cause. The condition leads to the partial or complete inability to voluntarily move facial muscles on the affected side of the face (Baugh et al., 2103).
Progression in Bell’s palsy is spontaneously favorable, with more than 70% complete resolution within 6 months (Berg et al., 2013) and more than 80% subtotal resolution (House-Brackmann grade I or II) (Peitersen, 2002). Prognosis is thus usually good, but in a frequent pathology with severe social impact if recovery is incomplete. Physical therapy is applied in Bell’s palsy persisting beyond the first months, to hasten recovery and limit sequelae. A recent meta-analysis of 12 studies for 872 patients reported high risk of bias due to variations in techniques and timing. However, it is clear that facial muscle rehabilitation improves facial function when Bell’s palsy fails to resolve (Teixeira et al., 2011).
There is no evidence to support the benefit or harm of physical therapy as a treatment for Bell’s palsy. The lack of standardized therapy modalities and protocols hampers the ability to make a recommendation regarding the use of physical therapy for patients with Bell’s palsy (Fieux et al., 2020; Bough et al., 2013). NMT application as an innovative modality treatment is able to provide positive effect using decompressive stimulate in the musculoskeletal, vascular, lymphatic and neurological systems (Blow, 2013). As the tapes form wrinkles and lift the skin, they facilitate venous and lymphatic drainage, improve blood circulation and relieve pain to bell’s palsy.
Case description
The patient, a student was 18-year-old woman who was, diagnosed with unilateral bell’s palsy of the left facial nerve and complete left facial paralysis. The initial physiotherapy evaluation was conducted 3 days following the onset of symptoms of left facial paralysis. The patient reported that her facial paralysis came on suddenly in the morning and was accompanied by pain in her left lateral neck and ear, decrease facial muscle strength and facial expression problem. She feels loss of eye blinking, difficulties to drink and chewing of foods, cannot give expression during talking. She was initially examined by neurologist in the hospital who prescribed a course of anti-viral, oral steroids, and referred to physiotherapy.
Neuro Muscular Taping (NMT) application
NMT application were designed with a principles NMT concept by Blow [Blow, 2012), focusing on tape to lymphatic decompression application in the neck, muscles decompression application in the side left of facial muscles, exercise using activation as NMT principles. NMT prescription was a decompression type, I strip with tape weight is depending on a target area, twice a day, for 4 times treatment for 30 minutes per session with application principles are position, fix, adhere, verify, and activate. First application was on the left side neck area according to the lymphatic path. The second and third application was to m. Frontalis and m. Orbicularis oculi. The fourth application done to facial muscles on the left side namely m. Risorius, m. Zygomaticum, m. Buccinator, m. Masseter, m. Levator Labii Superior, m. Levator anguli oris, and m. Temporalis. The details of the NMT application are summarized in Figure 1.
Exercise therapy applies, activation like as the principle of NMT application, that exercises carried out in areas given taping passively, active assisted, active by the herself to create the appearance of wrinkle that will bring a strong oxygenation effect. Exercise was also enhanced by minimal resistance to increase the strength of the weak side facial muscles beside that to stimulation of a number of nociceptors in the skin.
In this study NMT application was added home program education that patient done practicing pronunciation A I U E O every day, chewing gum, blow balloons, singing, and eye protection.
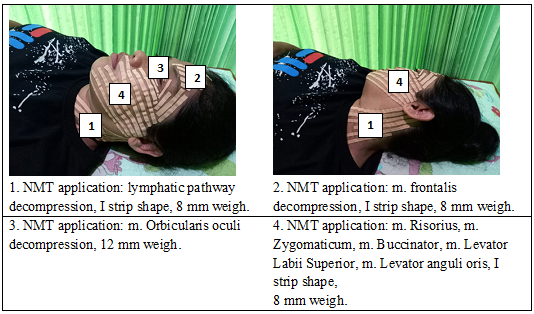
Figure 1: The details of the NMT application
Assessments and diagnosis
Assessments were performed before and after therapy with the fourth therapy and followed up 3 weeks after the program was completed. Physiotherapy evaluation further consisted of a qualitative of her pain/sensory problems, resting facial and neurological examination of the face, which revealed hypo-aesthetic response. Patient resting facial revealed severe asymmetry with a left sided droop. Voluntary movement of the left sided facial muscles was barely visible whereas the uninvolved right-sided facial muscles was clearly intact. The physiotherapist also performed active movement on the face. The patient’s pain/sensory problem and functional disability levels were evaluated using the numerical pain rating scale and the Ugo Fisch Scale, respectively.
The numerical pain rating (NRS) scale was used to rate the perceived pain on a scale of 0 (no pain) to 10 (the worst pain imaginable) (Lazaridou et al., 2018). To assess self-reported disability at baseline and to monitor treatment progress, the patient completed the Ugo Fisch Scale. The Ugo Fisch Scale is designed to provide the clinician with information regarded symmetrical of the face. The Ugo Fisch Scale consists of five subscales: rest, frowning, close eyes, smiling, whistling with the value of the movement performed were 20, 10, 30, 30, 10, respectively. The scores range from 0 (complete paralysis) to 100 (normal facial function). Assessment of the Ugo Fisch Scale for each subscale were 0% if zero muscles strength (complete asymmetry/no volunteer motion), 30% if poor muscles strength (healing towards asymmetry), 70% if fair muscles strength (partial healing towards symmetry), and 100% if normal muscles strength/complete symmetry).
Written informed consent to publication of this case report was obtained from the patient after describing the nature of assessments. Furthermore, Assessment results are used to formulate a diagnosis as in ICF model (WHO, 2001) (Figure 2).
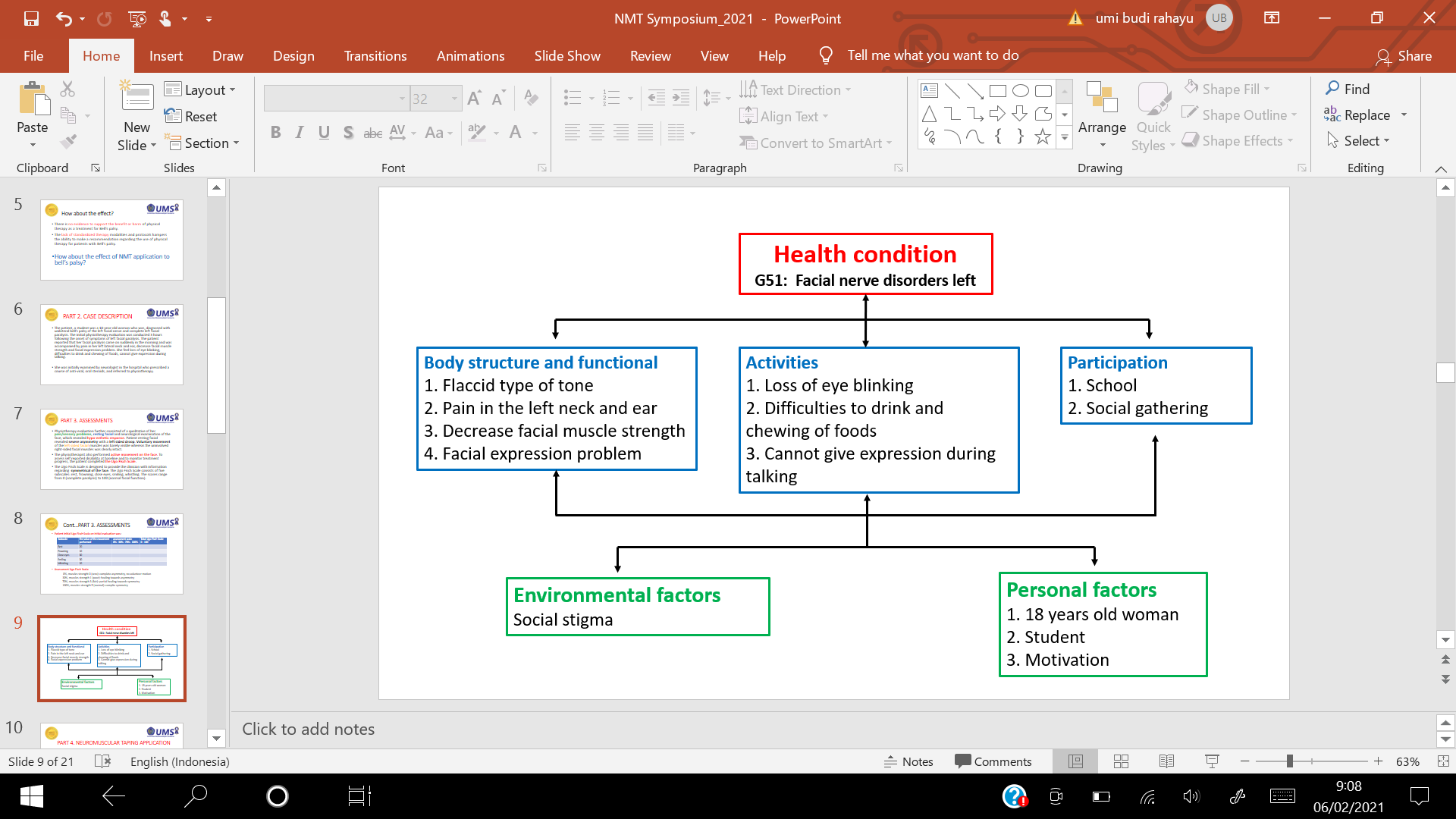
Figure 1: ICF model on facial nerve disorders
Results
A student diagnosed Bell’s Palsy was discharged 4 times treatment after NMT application as well as activation and home program education. She achieved significant pain, muscles strength and symmetrical of the face, with an improvement in the score of the NRS from 8.0 at the initial assessment to 2.0 after the for at the second treatment.
We also observed that after therapy there was an improvement in the condition with increased muscle strength characterized by symmetrical of the face, which was observed using The Ugo Fisch Scale. We
showed that the symmetrical of the face was 0 increased significantly after first therapy until fourth therapy to 4 is 18, 48, 71, 93, respectively as in Table 1 and Diagram 1. The follow-up after three weeks indicates that all complaints are not complained by the patient.
|
Subscales |
Before Treatment |
First treatment |
Second treatment |
Third treatment |
Fourth treatment |
|
Rest |
20 x 0% = 0 |
20 x 0% = 0 |
20 x 30% = 6 |
20 x 70% = 14 |
20 x 100% = 20 |
|
Frowning |
10 x 0% = 0 |
10 x 0% = 0 |
10 x 0% = 0 |
10 x 30% = 3 |
10 x 100% = 10 |
|
Close eyes |
30 x 0% = 0 |
30 x 30% = 9 |
30 x 70% = 21 |
30 x 100% = 30 |
30 x 100% = 30 |
|
Smiling |
30 x 0% = 0 |
30 x 30% = 9 |
30 x 70% = 21 |
30 x 70% = 21 |
30 x 100% = 30 |
|
Whistling |
10 x 0% = 0 |
10 x 0% = 0 |
10 x 0% = 0 |
10 x 30% = 3 |
10 x 30% = 3 |
|
Total |
0/100 |
18/100 |
48/100 |
71/100 |
93/100 |
Table 1: The Ugo Fisch Scale value as symmetrical facial indicator
Discussion
A person with bell's palsy is usually advised to take a break with various medications from the doctor because it will heal perfectly despite having a long time. Healing process can be gradual up to 6 months that will only be felt perfectly healed (Berg et al., 2013). However, as seen in this case report, inadequate reduction after given NMT application showed a faster time to overcome the pain/sensory problem around the left ear and neck. Elastic tape treatment using NMT concept is an innovative method. It’s a biomechanical therapy using decompressive stimulation to obtain positive effects in the musculoskeletal, vascular, lymphatic and neurological systems. As the tapes form wrinkles and lift the skin, they facilitate venous and lymphatic drainage, improve blood circulation, venous return, and relieve pain (Blow, 2012).
Rapid pain reduction is significantly associated with sensory-motor mechanisms and proprioceptive feedback in the brain (Laurie Lundy-Ekman, 2007). When elastic tape is an activated there will be eccentric and concentric movement of skin tissue and under the skin in the treatment area, then able to induce changes in the surrounding environment. Stimulates cutaneous mechanoreceptors and nociceptor and transmit exteroceptive and proprioceptive are able to stimulate CNS, further affecting muscle action response. Continuous stimulation becomes strong stimulates and trigger nerve impulses along the efferent nerve fibers. Related to the application of NMT in reducing pain and speeding up the treatment process of the planned series, it has been proven that there is an increase in the value of NPRS as well as the range of motion after I-shaped posterior neck decompression in cases of occipital neuralgia (Andi et al., 2019).
Further effects are to maintains a continuous relaxation effect and adequacy of oxygenation on muscle fibre. The application of elastic tape in the neck according to the lymphatic pathway is not only able to reduce pain but will also help drain fluid, while adequate oxygenation in the lesion facial muscles will accelerate the regeneration process. With the addition of exercises, tape activation, and home education programs (saying the font A I U E O every day, blowing balloons and chewing gum) showed an acceleration of the strength of the facial muscles indicated by the acceleration of facial symmetry (Diagram 1).
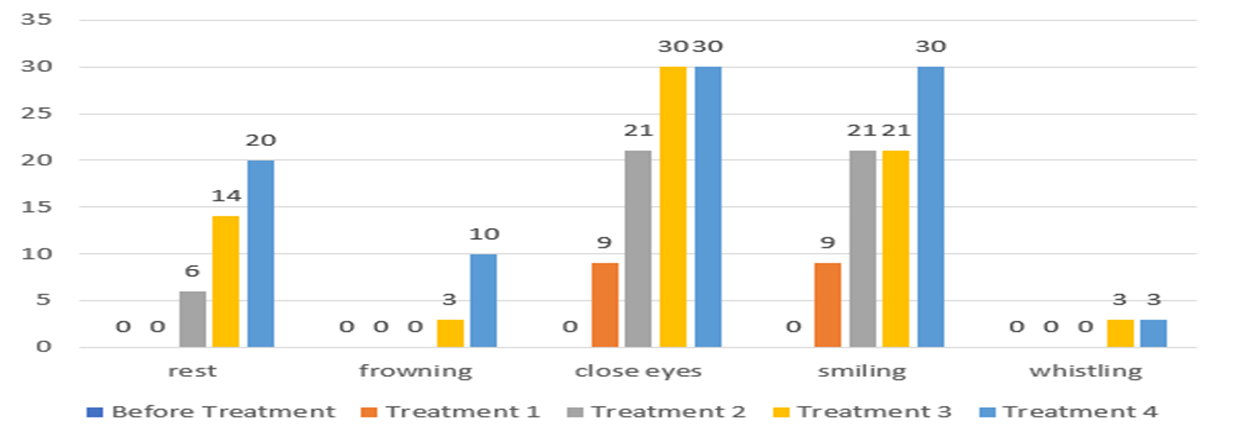
Diagram 1: Symmetrical face indicated strength of the facial muscles using the Ugo Fisch Scale
During the 4 times treatment, the patient showed significant improvement in the level of pain and symmetrical facial, as well as in function dan face expression. These findings may be associated with effect of NMT application in affecting oxygenation but also lymphatic flow in the treatment area. The patient could feel comfortable with the pain/sensory felt earlier after first treatment. Symmetry in the face also improves with the passage of treatment time. Tape elastic treatment applied will be very helpful in exercises and educational programs conducted by patients at home. This was shown to accelerate muscle strength on the lesion side and accelerate the symmetrical face indicated by the Ugo Fisch Scale value to 91 from a value of 100 after fourth treatment. Evaluation results in the follow up phase after 3 weeks showed that the patient was already feeling really improved. Efforts to improve therapy are also carried out with eye protection by using glasses to prevent irritation and doing the supporting thing of the patient's hobby of singing.
This indicates the acceleration of the healing process. Al Shalawi (2018), patient received six weeks of based physiotherapy service including proprioceptive exercise, trophic stimulator, transcutaneous electrical nerve stimulation, facial neuromuscular rehabilitation and home exercise programs. Patient showed improvement in pain reduction at numerical pain rating scale by 4 cm and improvement of facial expression by 55% in accordance to Synkinesis Assessment Questionnaire (SAQ). While, Engstrom et al. (2008) that without treatment, facial function is completely restored in approximately 70% of Bell’s palsy patients with complete paralysis within 6 months and as high as 94% of patients with incomplete paralysis; as many as 30% of patients do not recover completely.
These findings suggest that NMT applications with tape elastic decompression methods designed to help accelerate the recovery of bell's palsy patient problems such as pain/discomfort, muscle weakness and unsymmetrical face. Another important thing is to prevent further disability as a secondary symptom if it does not heal immediately. From this case it is recommended that NMT application can be done as early as possible for the purpose of oxygenation under the proper guidance of a physiotherapist. Future study recommendation that will be need to be do research with a larger number of samples.
Conclusion: NeuroMuscular Taping is a concept therapy by using elastic tape with decompression methods to give positive effect in Bell’s palsy, especially to speed up the loss of pain complaints and restore symmetry to the face, especially to provide a quick effect to increase pain and restore symmetry to the face.
Ethical approval
Not applicable. Written patient consent to publication of this case history was obtained.
Conflict of interest: None declared

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org