Clinical Research and Clinical Case Reports
OPEN ACCESS | Volume 7 - Issue 1 - 2026
ISSN No: 2836-2667 | Journal DOI: 10.61148/2836-2667/CRCCR


David Hana1*, Bijay Parajuli2, Marco Shaker3
1Department of Medicine, University of West Virginia, WV, USA
2Department of Medicine, Loyola University, Chicago, IL, USA
3Department of Medicine, Loyola University, Chicago, IL, USA
*Corresponding author: David Hana, Department of Medicine, University of West Virginia, WV, USA
Received: August 10, 2021
Accepted: August 14, 2021
Published: August 20, 2021
Citation: David Hana, Bijay Parajuli, Marco Shaker. “Levofloxacin-Induced Hypoglycemia in Insulin Dependent Diabetes Mellitus”. Clinical Research and Clinical Case Reports, 2(1); DOI: http;//doi.org/04.2021/1.1032
Copyright: © 2021 David Hana. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
,
Introduction
It is not uncommon for many antibiotics to induce hypoglycemia in diabetic and non-diabetic patients. Fluoroquinolones - Levofloxacin in specific - are on the top of the antibiotic list which is associated with glucose derangements and hypoglycemic events. Here is a 70 years old insulin-dependent diabetic gentleman who experienced hypoglycemic events after starting levofloxacin.
Case scenario
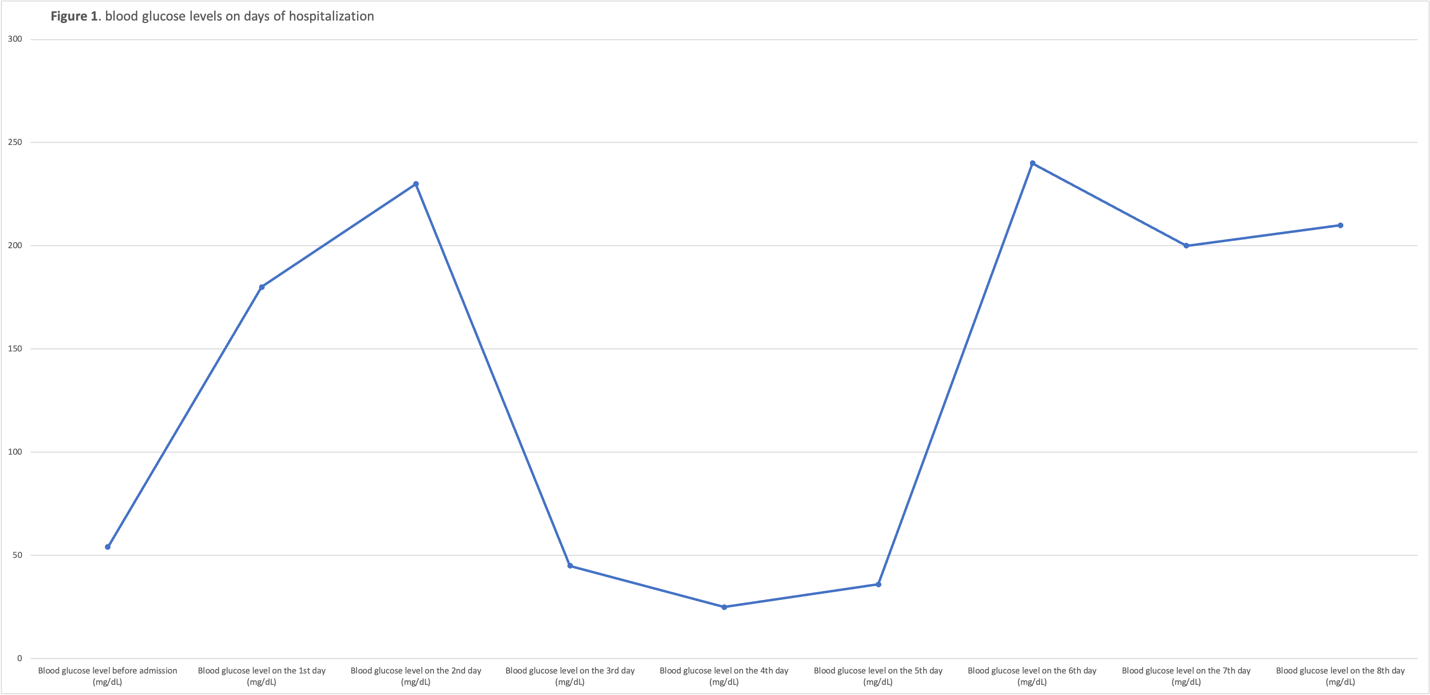
A 70-year-old patient with a history of hypertension, sacral decubitus ulcer associated with osteomyelitis (OM), and diabetes mellitus, presented from a nursing home (NH) for recent onset of hypoglycemic events and altered mental status. In the NH, the patient was on antibiotic therapy for OM (Levofloxacin, Cefepime, and Tigecycline), insulin therapy for 5 years, and heart failure therapy. On admission, the patient was afebrile, vital signs hemodynamically stable, point-of-care testing for glucose was 65 and dextrose 50% was given intravenously. On exam, the patient was alert and oriented x2, lethargic, the back exam showed a large stage 4 decubitus ulcer, otherwise was nonsignificant. Labs demonstrated evidence of chronic kidney disease and urinary tract infection. The patient has been admitted for further management of his diabetic regimen. Initially, the patient started on cefepime and vancomycin. On the third day, wound culture results were obtained from the NH and the patient started on Levofloxacin, Minocycline, and Linezolid. Then, the patient started experiencing multiple hypoglycemic events. The insulin regimen was cut down multiple times up to ¼ of his home regimen. After further discussion, levofloxacin has switched to ceftazidime on the 6th day of hospitalization. Since that time, no hypoglycemic events have been noted and the patient's mental status has improved (Figure 1).
Discussion
Fluoroquinolones use has been linked in multiple studies and case reports to dysglycemia including hypo and hyperglycemia. Fluoroquinolones cause hypoglycemia by increasing insulin secretion in a dose-dependent manner through inhibition of adenosine 5'-triphosphate potassium ion channels. On the other side, it can also cause hyperglycemia but the mechanism is still unclear. We will focus in our discussion on hypoglycemia. The most common fluoroquinolones that cause hypoglycemic events are gatifloxacin, levofloxacin, and moxifloxacin. Gatifloxacin was withdrawn from the market in 2006 for the same reason. [1, 2]
Levofloxacin-induced hypoglycemic occurs predominantly in type II diabetes mellitus (DM) on oral hypoglycemic therapy, mainly sulfonylureas. [3, 4] However, hypoglycemia has been also reported in several patients without a history of DM or any glucose-lowering medication. [5-7] Other confounding factors for hypoglycemia in our patient includes severe infection, low oral intake, and chronic kidney disease (CKD). [2, 8] The low oral intake has been excluded and the patient was receiving a renally appropriate dose of levofloxacin. Additionally, the patient didn’t develop any hypoglycemic events when he wasn’t on levofloxacin, even though he still had severe infection and CKD.
Theoretically, a patient with Type 1 DM or insulin-dependent type 2 DM can’t develop hypoglycemia after levofloxacin use, but hypoglycemia has been reported in insulin-dependent patients in multiple studies before. A retrospective cohort study by Lodise et. al. demonstrated that 20% of the patients who developed hypoglycemic events after fluoroquinolones intake were insulin-dependent diabetics. [9] Even further, a retrospective medical record review by LaPlante et. al. showed that the presence of diabetes and diabetic regimen with either insulin therapy or sulfonylureas are independent predictors for developing dysglycemic events after quinolones intake. [10] These patients might still have reserve pancreatic function leading to increased insulin secretion after levofloxacin administration.
The incidence of levofloxacin-induced hypoglycemia is rare. The incidence risk according to the manufacturing is < 0.01%.[5] A retrospective cohort study among diabetic and nondiabetic patients by Aspinall et. al. demonstrated that the crude incidence rate of severe levofloxacin-induced hypoglycemia is 0.19 cases per 1000 persons. [1] And according to a population-based cohort study among diabetic patients in Taiwan, the absolute risk for hypoglycemia after levofloxacin is 9.3 cases per 1000 persons. [2] Additionally, LaPlante et. al. did not find any significant increase in dysglycemic events among the ambulatory populations who consumed fluoroquinolones. [10]
Conclusion
Despite the current understanding of the mechanism by which levofloxacin-induced hypoglycemia occurs, the incidence of hypoglycemic events in insulin-dependent diabetic patients has been reported before and in the current case. Concisely, we should be attentive to the glucose level after prescribing levofloxacin in all patients. We agree for special consideration in diabetic patients on glucose-lowering agents. But still, it can happen in non-diabetic patients and insulin-dependent diabetic patients. Although the incidence is rare, the consequences are significant and life-threatening.












Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org