Clinical Research and Clinical Case Reports
OPEN ACCESS | Volume 7 - Issue 1 - 2026
ISSN No: 2836-2667 | Journal DOI: 10.61148/2836-2667/CRCCR


Sajjad Hussain
Consultant Surgeon, District Hospital Kargil. U.T Ladakh, India
*Corresponding authors: Sajjad Hussain, Consultant Surgeon, District Hospital Kargil. U.T Ladakh, India
Received: March 28, 2021
Accepted: April 06, 2021
Published: April 09, 2021
Citation: Sajjad Hussain. “Internal Supra-Vesical hernia: A very rare cause of small bowel obstruction and review of literature”. Clinical Research and Clinical Case Reports, 1(1); DOI: http;//doi.org/04.2021/1.1002.
Copyright: © 2021 Sajjad Hussain. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Internal Supravesical hernia is an unusual type of hernia. Small bowel obstruction due to the Supravesical hernia is very rarely seen. Clinical diagnosis of this hernia is almost never suspected before surgery; hence familiarity with this condition as well as the anatomy of the Supravesical fossa may allow preoperative diagnosis by CT in a few instances.
Introduction:
Internal Supravesical hernia is one of the rarest types of hernia. Supravesical hernia occurs via Supravesical fossa which is a triangular space, bounded laterally by the median umbilical ligament covering the remnants of the left or right umbilical arteries. The fossa is medially bordered by the Uracus (medial urachial fold) and below by the peritoneal fold that separates the anterior abdominal wall from the dome of the bladder (Cooper’s ligament) [1]. A bulge may protrude through the Supravesical fossa, which may develop in different directions. The protrusions that emerge through the cranial aspect of the fossa usually generate external Supravesical hernia, while those expanding into the inferior area generally penetrate the prevesical space of Retzius (behind the pubic bone) resulting in internal Supravesical hernias [2]. In brief, these two kinds of hernias simply differ in the path of the protrusion: an internal hernia doesn’t cross the abdominal wall and remains restricted in the preperitoneal space, presenting with the prevesical, paravesical, lateral or intravesical variant [3]. An external hernia in this fossa can form as a result of a defect in the integrity of the transverses abdominis muscle and fascia transversalis and hence pass through the abdominal wall expanding into the inguinal canal medially of the medial inguinal fossa and may present as one of the variant of direct inguinal hernia [4].
Supravesical hernias are acquired hernias and they are sometimes associated with the inguinal hernias [5]. The majority of the patients with internal Supravesical hernia present with acute obstructive symptoms caused by small bowel strangulation [6]. The low recognition of internal Supravesical hernia due to lack of awareness of this rare condition makes preoperative diagnosis very difficult, although characteristic CT findings have been reported. I report a case of a 65 year old man who presented with the small bowel obstruction. Highlighting and further studying this rare condition could probably help surgeons in adequately identifying small bowel obstruction due to internal Supravesical hernia, and thus help in adopting an appropriate strategy for accurate preoperative diagnosis and surgical treatment.
Case Report:
An elderly man presented with a history of colicky abdominal pain and vomiting of 5 days duration. He had a history of exploratory laparotomy for duodenal perforation peritonitis some 20-30 years back. He was having left hemi-paresis due to a stroke 2 years back. He also had history of left uncomplicated inguinal hernia for the last 3 years. On examination, he was dehydrated with a heart rate of 100bpm, blood pressure of 120/86mmHg, and a temperature of 370C. His abdomen was distended, mildly tender and having a previous long midline incision scar. There was also a small, direct, reducible, uncomplicated, left inguinal hernia. Blood tests showed leucocytosis. Plain film radiography showed distended small-bowel loops with air-fluid levels consistent with a small-bowel obstruction. Adhesional small-bowel obstruction was suspected clinically. C.T scan abdomen showed dilated small bowel loops. The coronal C.T image (figure 1) demonstrated a U – shaped bowel loop with a sac – like appearance, on the right side of lower abdomen just over the urinary bladder and pressing it. The axial C.T image (figure 2) showed two transition points of the pseudo-encapsulated small bowel loop above the urinary bladder. The patient underwent exploratory laparotomy and intra-operatively small-bowel obstruction due to right internal Supravesical hernia (Figure 3), was found. The closed loop obstruction had caused strangulation (Figure 4) and hence resection anastomosis of involved ileal loop was done due to doubtful viability. The hernia defect (Figure 5) was closed with interrupted 1/0 Prolene stitches. The patient recovered uneventfully and was discharged on 8th postoperative day.
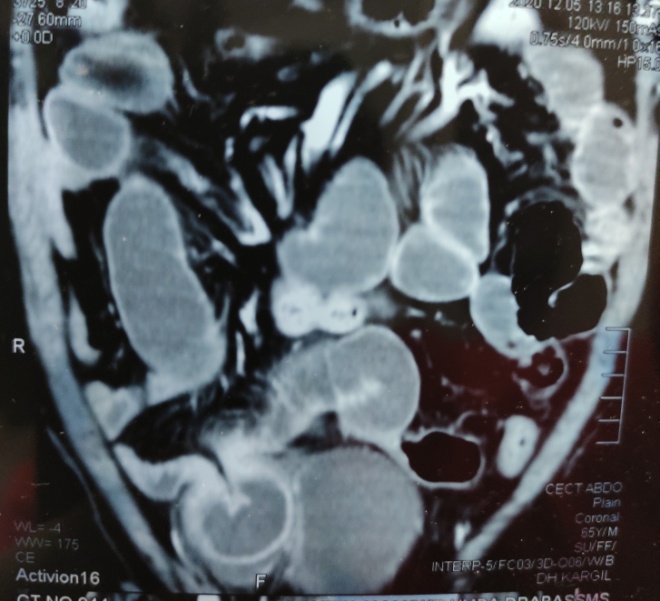
Figure 1. Coronal CT showing a U-shaped bowel loop with a sac-like appearance, pressing the urinary bladder.
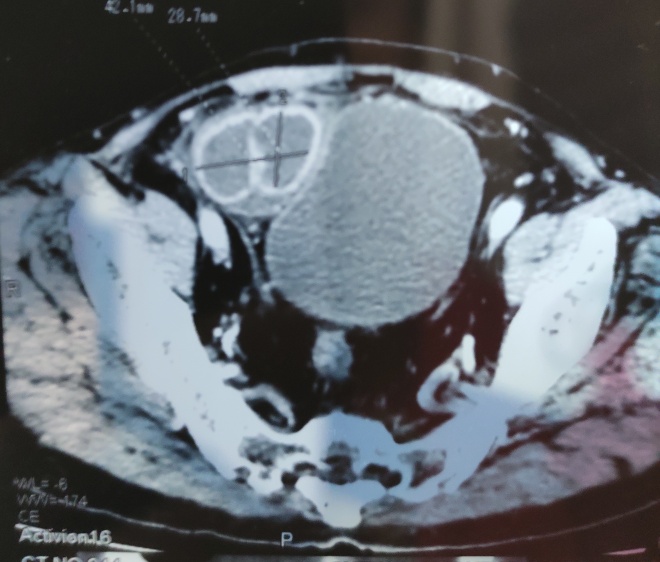
Figure 2. Axial CT scan showing two transition points of the pseudo-encapsulated small bowel loop.
Discussion:
Small bowel obstruction due to the Supravesical hernias is very rarely seen and till date, less than 100 cases have only been reported in literature after the report of first such case by Astely Cooper in 1804, followed by Ring in 1814 [7].
Skandalakis et al. proposed the simpler terms “anterior Supravesical”, “right or left lateral Supravesical”, and “posterior Supravesical” depending on whether the hernia passes in front of, beside, or behind the bladder, respectively [8]. Internal Supravesical hernia occupies the prevesical space of Retzius and in turn can be prevesical, para-vesical, lateral or intra-vesical due to weakened bladder apex by a defective closure of the Uracus, leading to herniation of the diverticulum directly into the bladder [9].It has been inferred that Supravesical hernia is an acquired disease caused by diminution of preperitoneal fat due to various factors ( aging, malnutrition, and disease) or by dysraphism between cooper’s ligament and the transversal fascia due to subperitoneal tissue-fibrillary contraction after inflammation [10]. Another theory is that Supravesical hernia is caused by an extraordinarily large medial umbilical fold congenitally that creates a pocket above the bladder [11]. Ozturk et al. indicted that there was a developmental anomaly of the urinary system in their cadaveric case [12]. However the pathogenesis has not yet been clarified.

Figure 3. Intraoperative view of closed loop obstruction of ileal segment in the hernia sac.
C.T scan is a reliable imaging modality for diagnosis of internal Supravesical hernia. The herniated intestine usually shows a sac-like appearance, which is a common imaging feature of an internal Supravesical hernia. Internal hernias, including internal Supravesical hernias, frequently cause closed loop obstruction and subsequent bowel strangulation [13]. Typical C.T scan findings of a dilated bowel loop trapped in the Supravesical fossa compressing the bladder, as in this case, have been described in hope of improving accuracy in preoperative diagnosis. But the lack of awareness to this rare condition is a big obstacle in achieving this goal [14]. Patients are usually diagnosed with small bowel obstruction/ strangulation (47%) or internal hernias (17.6%), and undergo urgent surgery. Hence, the low accuracy in pre-operative diagnosis does not actually have a great impact on mortality. However, it frequently involves necrosis of the incarcerated bowel, with 6 out of 17 (35%) in our literature review and so awareness of the importance of urgent surgical attention is essential.
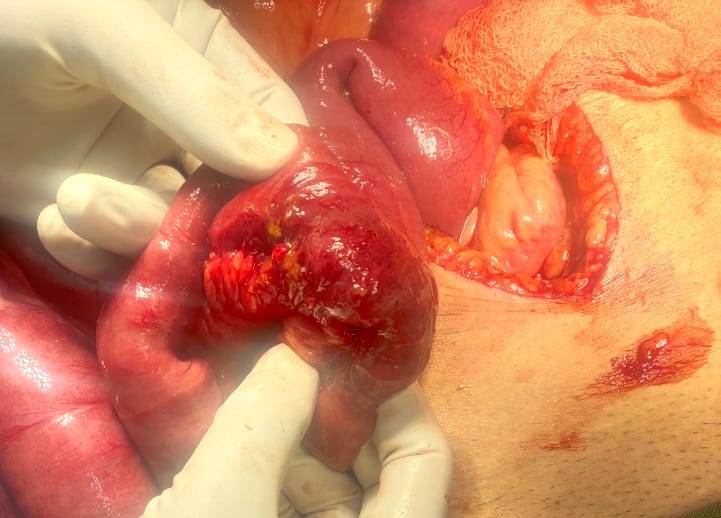
Figure 4. Showing strangulated closed loop after releasing from the hernia sac
There is no gold standard surgical procedure for internal supravesical hernia. Reduction of the incarcerated bowel is an essential step, followed by closure of the hernia orifice by using continuous or interrupted non-absorbable suture. Freshening the edges of the ring can be done. Removal of the hernia sac is not essential as sac dissection is dangerous with risk of bladder damage. [3]. Almost all previous reports involved open laparotomy, where as a few cases were repaired laparoscopically [6] and in only one case surgery was done by anterior approach [10]. Laparoscopic approach may be helpful in patients with stable hemodynamic parameters and in patients with early diagnosis by C.T scan, with limited intestinal distension [15].

Figure 5. Intraoperative view of internal supra-vesical hernia sac/ hernia defect.
Conclusion:
The diagnosis of internal supravesical hernia is usually made per-operatively. This case illustrates the difficulty in diagnosing this rare type of internal supravesical hernia and calls attention to the entity as an unusual cause of small bowel obstruction.
Conflict of Interest:
The author has no financial or any conflict of interest to declare.












Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org