
Noor Fatima Shahid 1, Saima Shokat 2, Samreen Riaz 3,4
1Pakistan Kidney and liver Institute. Lahore, Pakistan
1,3Department of Microbiology and Molecular Genetics, University of the Punjab, Lahore. Pakistan.
2Government College University Lahore.
4Academy of Family Physician of Pakistan.
*Corresponding author: Samreen Riaz, Government College University Lahore.
*Corresponding author: Samreen Riaz, Government College University Lahore.
Received date: January 04, 2021
Accepted date: January 20, 2021
published date: February 10, 2021
Citation: Noor F Shahid, Shokat S, Riaz S. “Coronoa Virus Pandemic: New Environmental Pollutant.’’. Endocrinology and Surgical Endocrinology, 2(1); DOI: http;//doi.org/03.2021/1.1002.
Copyright: © 2021 Samreen Riaz. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
Background: Patients with COVID-19 who have elevated blood sugar levels without a previous diagnosis of diabetes may be at a high risk of death and an increased risk of severe complications from the infectious disease, a new study says. Objective: We aimed to briefly review the general characteristics of the novel coronavirus (SARS-CoV-2) and provide a better understanding of the coronavirus disease (COVID-19) in people with diabetes, and its management. Method: We searched for articles in PubMed and Google Scholar databases till 02 October 2020, with the following Results: The clinical spectrum of COVID-19 is heterogeneous, ranging from mild flu-like symptoms to acute respiratory distress syndrome, multiple organ failure and death. Older age, diabetes and other comorbidities are reported as significant predictors of morbidity and mortality. Chronic inflammation, increased coagulation activity, immune response impairment, and potential direct pancreatic damage by SARS-CoV-2 might be among the underlying mechanisms of the association between diabetes and COVID-19. No conclusive evidence exists to support the discontinuation of angiotensin-converting enzyme inhibitors (ACEI), angiotensin receptor blockers or thiazolidinedione’s because of COVID-19 in people with diabetes. Caution should be taken to potential hypoglycemic events with the use of chloroquine in these subjects. Patient tailored therapeutic strategies, rigorous glucose monitoring and careful consideration of drug interactions might reduce adverse outcomes. Conclusions: Suggestions are made on the possible pathophysiological mechanisms of the relationship between diabetes and COVID-19, and its management. No definite conclusions can be made based on current limited evidence. Further research regarding this relationship and its clinical management is warranted.
Introduction
Corona Virus: Structure and Forms:
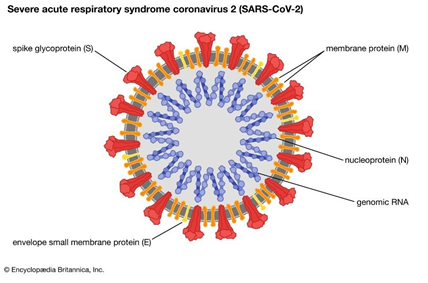
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a novel severe acute respiratory syndrome coronavirus, first isolated from three people with pneumonia connected to the cluster of acute respiratory illness cases in Wuhan. SARS-CoV-2 is closely related to the original SARS-CoV. It is thought to have a zoonotic origin. Genetic analysis has revealed that
1.1 The coronavirus genetically clusters with the genus Beta coronavirus, in subgenus Sarbecovirus (lineage B) together with two bat-derived strains. It is 96% identical at the whole genome level to other bat coronavirus samples (Bat Cov RaTG13). In February 2020, Chinese researchers found that there is only one amino acid difference in certain genome sequences between the viruses found in pangolins and those from humans, however, whole genome comparison to date found at most 92% of genetic material shared between pangolin coronavirus and SARS-CoV-2, which is insufficient to prove pangolins to be the intermediate host.

What is Coronavirus COVID -19 ?
1.2 Coronavirus mechanism of actions:
The virus is primarily spread between people similar to influenza, via respiratory droplets from coughing and sneezing. It is considered most contagious when people are symptomatic, although transmission may be possible before symptoms appear. The time between exposure and symptom onset is typically five days, but may range from two to fourteen days. Common symptoms include fever, cough, and shortness of breath. Complications may include pneumonia and acute respiratory distress syndrome. Currently, there is no vaccine or specific antiviral treatment; efforts consist of symptom alleviation and supportive therapy. Recommended preventive measures include handwashing, covering the mouth when coughing, maintaining distance from other people (particularly those who are unwell), and monitoring and self-isolation for fourteen days for people who suspect they are infected. The primary mode of transmission is via respiratory droplets that people exhale, for example when coughing or sneezing. Droplets stay suspended in the air for only a short time but may stay viable and contagious on a metal, glass or plastic surface. The stability of the SARS-CoV-2 virus in the air and on various surfaces is believed to be comparable to that of other coronaviruses, some of which can survive for up to nine days at room temperature. Its similarity to SARS-CoV-1 in particular was confirmed in laboratory tests that found both viruses could survive up to or beyond 72 hours on plastic and stainless steel. A survey of research on the inactivation other coronaviruses using various biocidal agents suggests that disinfecting surfaces contaminated with SARS-CoV-2 may also be achieved using similar solutions, including 62–71% ethanol, 50–100% isopropanol, 0.1% sodium hypochlorite (after one minute), 0.5% hydrogen peroxide, and 0.2–7.5% povidone-iodine; benzalkonium chloride and chlorhexidine gluconate are less effective. The WHO has stated that the risk of spread from someone without symptoms is "very low". However, if someone has beginning symptoms and a mild cough, there is a risk of transmission.COVID-19 has a higher transmission rate and a greater risk of mortality in comparison with influenza. Although the majority of the patients are believed to have a favorable outcome, older people with underlying diseases may have a poor prognosis. Diabetes mellitus is one of the most common conditions among the elderly and contributes greatly to the morbidity worldwide. Moreover, numerous studies have shown that diabetic patients are more susceptible to various pathogens, such as Mycobacterium tuberculosis, Streptococcus pneumonia, and Staphylococcus aureus. Several retrospective studies in Wuhan indicated that diabetes was one of the most prevalent comorbidities in COVID-19 patients, and suggested that diabetics were probably more susceptible to SARS-CoV-2 and these patients might have a worse prognosis.

Figure 2: Symptoms of Coronavirus Disease 2019
1.1 Symptoms of Coronavirus:
Symptoms of COVID-19 are non-specific and those infected may either be asymptomatic or develop flu like symptoms such as fever, cough, fatigue, shortness of breath, or muscle pain. The typical signs and symptoms and their prevalence, are shown in the corresponding table. Further development can lead to severe pneumonia, acute respiratory distress syndrome, sepsis, septic shock and death. Some of those infected may be asymptomatic, returning test results that confirm infection but show no clinical symptoms, so researchers have issued advice that those with close contact to confirmed infected people should be closely monitored and examined to rule out infection. The usual incubation period (the time between infection and symptom onset) ranges from one to fourteen days; it is most commonly five days. In one case, it had an incubation period of 27 days.
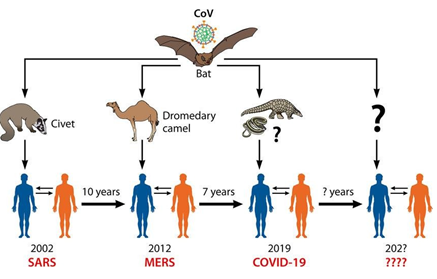
Figure 3.Coronavirus is the most prominent example of an emerging virus that has crossed the species barrier from wild animals to humans, like SARS and MERS.
1.2 Origin of Coronavirus:
The first known case of the novel coronavirus was traced back to 1 December 2019 in Wuhan, Hubei, China. A later unconfirmed claim, citing Chinese government documents, suggests that the first victim was a 55-year-old man who fell ill on 17 November 2019.[under discussion] Within the next month, the number of coronavirus cases in Hubei gradually increased to a couple of hundred, before rapidly increasing in January 2020. On 31 December 2019, the virus had caused enough cases of unknown pneumonia to be reported to health authorities in Wuhan, the capital of Hubei province, China, and an investigation into the illness began early in the following month. These were mostly linked to the Huanan Seafood Wholesale Market, which also sold live animals, consequently the virus is thought to have a zoonotic origin. During the early stages, the number of cases doubled approximately every seven and a half days. In early and mid-January 2020, the virus spread to other Chinese provinces, helped by the Chinese New Year migration, with Wuhan being a transport hub and major rail interchange in China; infected people quickly spread throughout the country. On 20 January, China reported nearly 140 new cases in a day, including two people in Beijing and one in Shenzhen. Later official data shows that 6,174 people had already developed symptoms by 20 January 2020. On 30 January, the WHO declared the outbreak to be a Public Health Emergency of International Concern. On 24 February, its director, Tedros Adhanom, warned that the virus could become a global pandemic due to increasing numbers of cases outside China. On 13 March, the WHO declared Europe to be the new center of the pandemic, after the rate of new cases in Europe surpassed those recorded in other regions of the world apart from China. By 16 March 2020, the total number of cases reported around the world outside China had exceeded that of Mainland China. As of 18 March 2020, over 204,000 cases have been reported worldwide; more than 8,200 people have died; and over 82,000 have recovered. There is thought to be a substantial underreporting of cases, particularly of cases with milder symptoms or no symptoms. As of 29 February, apart from mainland China, the epidemic had spread to several other countries around the world, with the most affected being South Korea, Italy and Iran. National response measures have included containment measures such as quarantines and curfews.
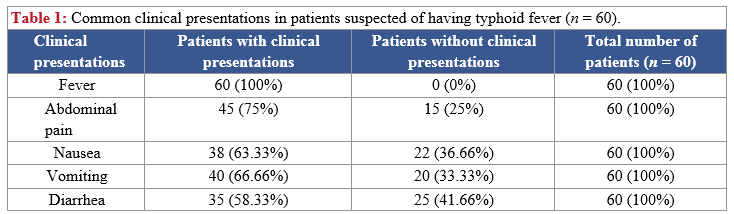
 Table 1: Common clinical presentations in patients suspected of having typhoid fever (n = 60).
Table 1: Common clinical presentations in patients suspected of having typhoid fever (n = 60).
Coronavirus Classification:
1.3 Severe acute respiratory syndrome coronavirus 1 (SARS-CoV-1)
Severe acute respiratory syndrome (SARS) is the disease caused by SARS-CoV-1. It causes an often severe illness and is marked initially by systemic symptoms of muscle pain, headache, and fever, followed in 2–14 days by the onset of respiratory symptoms, mainly cough, dyspnea, and pneumonia. Another common finding in SARS patients is a decrease in the number of lymphocytes circulating in the blood. Severe acute respiratory syndrome (SARS) is a viral respiratory disease of zoonotic origin caused by severe acute respiratory syndrome coronavirus (SARS-CoV or SARS-COV-1), the first-identified strain of the SARS coronavirus species severe acute respiratory syndrome- related coronavirus (SARSr-CoV). The syndrome caused the 2002–2004 SARS outbreak. In late 2017, Chinese scientists traced the virus through the intermediary of Asian palm civets to cave-dwelling horseshoe bats in Yunnan. SARS was a relatively rare disease; at the end of the epidemic in June 2003, the incidence was 8,422 cases with a case fatality rate (CFR) of 11%. No cases of SARS- CoV have been reported worldwide since 2004. In 2019, the related virus strain severe acute respiratory syndrome coronavirus 2 (SARS-COV-2) was discovered. This new strain causes COVID-19, a disease which brought about the COVID-19 pandemic.
This article is about the virus strain that causes SARS. For the strain that causes COVID-19, see severe acute respiratory syndrome coronavirus 2. For the species to which both strains belong, see severe acute respiratory syndrome–related coronavirus. Severe acute respiratory syndrome coronavirus (SARS-CoV or SARS-CoV-1) is a strain of virus that causes severe acute respiratory syndrome (SARS).It is an enveloped, positive-sense, single-stranded RNA virus
which infects the epithelial cells within the lungs. The virus enters the host cell by binding to angiotensin-converting enzyme 2.It infects humans, bats, and palm civets. On 16 April 2003, following the outbreak of SARS in Asia and secondary cases elsewhere in the world, the World Health Organization (WHO) issued a press release stating that the coronavirus identified by a number of laboratories was the official cause of SARS. The Centers for Disease Control and Prevention (CDC) in the United States and National Microbiology Laboratory (NML) in Canada identified the SARS-CoV-1 genome in April 2003.Scientists at Erasmus University in Rotterdam, the Netherlands, demonstrated that the SARS coronavirus fulfilled Koch's postulates thereby confirming it as the causative agent. In the experiments, macaques infected with the virus developed the same symptoms as human SARS victims. A similar virus was discovered in January, 2020. This virus, named Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-
2) is the causative pathogen of the ongoing COVID-19 pandemic. In the SARS outbreak of 2003, about 9% of patients with confirmed SARS-CoV-1 infection died. The mortality rate was much higher for those over 60 years old, with mortality rates approaching 50% for this subset of patients.
Figure
1.5 History of Sars CoV-1
On 17 March 2003, WHO established a global network of leading laboratories to collaborate in the identification of the causative agent of SARS .Early on, labs in the network narrowed the search to members of the paramyxovirus and coronavirus families. Early findings shared by the labs pointed to coronaviruses with increasing consistency. On 21 March, scientists from the University of Hong Kong announced the isolation of a new virus that was strongly suspected to be the causative agent of SARS. On 12 April, scientists working at the Michael Smith Genome Sciences Centre in Vancouver finished mapping the genetic sequence of a coronavirus believed to be linked to SARS. The team was led by Marco Marra and worked in collaboration with the British Columbia Centre for Disease Control and the National Microbiology Laboratory in
Winnipeg, Manitoba, using samples from infected patients in Toronto. The map, hailed by the WHO as an important step forward in fighting SARS, is shared with scientists worldwide via the GSC website (see below). Donald Low of Mount Sinai Hospital in Toronto described the discovery as having been made with "unprecedented speed‖. The sequence of the SARS coronavirus has since been confirmed by other independent groups. Molecular epidemiological research demonstrated the virus of 2002–2003 south China outbreak and the virus isolated in the same area in late 2003 and early 2004 outbreaks are different, indicating separate species- crossing events. The phylogeny of the outbreak strains shows that the southwestern provinces including Yunnan, Guizhou and Guangxi compare to the human SARS-CoV-1 better than those of the other provinces, but the viruses' evolution is a product of the host interaction and particularity.
In late May 2003, studies from samples of wild animals sold as food in the local market in Guangdong, China, found a strain of SARS coronavirus could be isolated from masked palm civets (Paguma sp.), but the animals did not always show clinical signs. The preliminary conclusion was the SARS virus crossed the xenographic barrier from palm civet to humans, and more than 10,000 masked palm civets were killed in Guangdong Province. The virus was also later found in raccoon dogs (Nyctereuteus sp.), ferret badgers (Melogale spp.), and domestic cats. In 2005, two studies identified a number of SARS-like coronaviruses in Chinese bats. Although the bat SARS virus did not replicate in cell culture, in 2008, American researchers altered the genetic structure of bat SARS virus with the human receptor binding domain both in the bat virus and in the mice which demonstrated how zoonosis might occur in evolution. Phylogenetic analysis of these viruses indicated a high probability that SARS coronavirus originated in bats and spread to humans either directly or through animals held in Chinese markets. The bats did not show any visible signs of disease, but are the likely natural reservoirs of SARS-like coronaviruses. In late 2006, scientists from the Chinese Centre for Disease Control and Prevention of University of Hong Kong and the Guangzhou Centre for Disease Control and Prevention established a genetic link between the SARS coronavirus appearing in civets and humans, confirming claims that the virus had jumped across species.
Table
|
|
Cumulative number of cases |
|
Status |
|
|
|
|
|||||
|
A r e a s |
Female |
Male |
Total |
Median age (range) |
Number of cases currently hospitalized |
Number of cases recovered |
Number of deaths |
CFR (%) 1 |
Number of imported cases (%) |
Number of HCW affected (%) |
Date onset first probable case |
Date onset last probable case |
|
Australia |
4 |
2 |
6 |
15 (1-45) |
0 |
6 |
0 |
0 |
6 (100) |
0 (0) |
24-Mar-03 |
1-Apr-03 |
|
Brazil |
1 |
|
1 |
4 |
0 |
1 |
0 |
0 |
1 (100) |
0 (0) |
3-Apr-03 |
3-Apr-03 |
|
Canada |
151 |
100 |
251 |
49 (1-98) |
10 |
200 |
41 |
17 |
5 (2) |
108 (43) |
23-Feb-03 |
12-Jun-03 |
|
China |
Pending |
Pending |
5327 |
Pending |
29 |
4949 |
349 |
7 |
NA |
1002 (19) |
16-Nov-02 |
25-Jun-03 |
|
China, Hong Kong Special Administrative Region |
977 |
778 |
1755 |
40 (0-100) |
7 |
1448 |
300 |
17 |
NA |
386 (22) |
15-Feb-03 |
31- May- 03 |
|
China, Macao Special Administrative Region |
0 |
1 |
1 |
28 |
0 |
1 |
0 |
0 |
1 (100) |
0 (0) |
5-May-03 |
5-May-03 |
|
China, Taiwan |
349 3 |
319 3 |
665 |
46 (2-79) |
10 |
475 |
180 |
27 |
50 (8) |
86 (13) |
25-Feb-03 |
15-Jun-03 |
|
Colombia |
1 |
0 |
1 |
28 |
0 |
1 |
0 |
0 |
1 (100) |
0 (0) |
2-Apr-03 |
2-Apr-03 |
|
Finland |
0 |
1 |
1 |
24 |
0 |
1 |
0 |
0 |
1 (100) |
0 (0) |
30-Apr-03 |
30-Apr-03 |
|
France |
1 |
6 |
7 |
49 (26 - 61) |
0 |
6 |
1 |
14 |
7 (100) |
2 2 (29) |
21-Mar-03 |
3-May-03 |
|
Germany |
4 |
5 |
9 |
44 (4-73) |
0 |
9 |
0 |
0 |
9 (100) |
1 (11) |
9-Mar-03 |
6-May-03 |
|
India |
0 |
3 |
3 |
25 (25-30) |
0 |
3 |
0 |
0 |
3 (100) |
0 (0) |
25-Apr-03 |
6-May-03 |
|
Indonesia |
0 |
2 |
2 |
56 (47-65) |
0 |
2 |
0 |
0 |
2 (100) |
0 (0) |
6-Apr-03 |
17-Apr-03 |
|
Italy |
1 |
3 |
4 |
30.5 (25-54) |
0 |
4 |
0 |
0 |
4 (100) |
0 (0) |
12-Mar-03 |
20-Apr-03 |
|
Kuwait |
1 |
0 |
1 |
50 |
0 |
1 |
0 |
0 |
1 (100) |
0 (0) |
9-Apr-03 |
9-Apr-03 |
|
Malaysia |
1 |
4 |
5 |
30 (26-84) |
0 |
3 |
2 |
40 |
5 (100) |
0 (0) |
14-Mar-03 |
22-Apr-03 |
|
Mongolia |
8 |
1 |
9 |
32 (17-63) |
0 |
9 |
0 |
0 |
8 (89) |
1 (11) |
31-Mar-03 |
6-May-03 |
|
New Zealand |
1 |
0 |
1 |
67 |
0 |
1 |
0 |
0 |
1 (100) |
|
20-Apr-03 |
20-Apr-03 |
|
Philippines |
8 |
6 |
14 |
41 (29-73) |
0 |
12 |
2 |
14 |
7 (50) |
4 (29) |
25-Feb-03 |
5-May-03 |
|
Republic of Ireland |
0 |
1 |
1 |
56 |
0 |
1 |
0 |
0 |
1 (100) |
0 (0) |
27-Feb-03 |
27-Feb-03 |
|
Republic of Korea |
0 |
3 |
3 |
40 (20-80) |
0 |
3 |
0 |
0 |
3 (100) |
0 (0) |
25-Apr-03 |
10- May- 03 |
|
Romania |
0 |
1 |
1 |
52 |
0 |
1 |
0 |
0 |
1 (100) |
0 (0) |
19-Mar-03 |
19-Mar-03 |
|
Russian Federation |
0 |
1 |
1 |
25 |
1 |
0 |
0 |
|
NA |
0 (0) |
5-May-03 |
5-May-03 |
|
Singapore |
161 |
77 |
238 |
35 (1-90) |
0 |
205 |
33 |
14 |
8 (3) |
97 (41) |
25-Feb-03 |
5-May-03 |
|
South Africa |
0 |
1 |
1 |
62 |
0 |
0 |
1 |
100 |
1 (100) |
0 (0) |
3-Apr-03 |
3-Apr-03 |
|
Spain |
0 |
1 |
1 |
33 |
0 |
1 |
0 |
0 |
1 (100) |
0 (0) |
26-Mar-03 |
26-Mar-03 |
|
Sweden |
1 |
2 |
3 |
33 |
0 |
3 |
0 |
0 |
3 (100) |
0 (0) |
|
|
|
Switzerland |
0 |
1 |
1 |
35 |
0 |
1 |
0 |
0 |
1 (100) |
0 (0) |
9-Mar-03 |
9-Mar-03 |
|
Thailand |
5 |
4 |
9 |
42 (2-79) |
0 |
7 |
2 |
22 |
9 (100) |
1 2 (11) |
11-Mar-03 |
27- May- 03 |
|
United Kingdom |
2 |
2 |
4 |
59 (28-74) |
0 |
4 |
0 |
0 |
4 (100) |
0 (0) |
1-Mar-03 |
1-Apr-03 |
|
United States |
16 |
17 |
33 |
36 (0-83) |
7 |
26 |
0 |
0 |
31 (94) |
1 (3) |
9-Jan-03 |
13-Jul-03 |
|
Viet Nam |
39 |
24 |
63 |
43 (20-76) |
0 |
58 |
5 |
8 |
1 (2) |
36 (57) |
23-Feb-0 |
14-Apr-03 |
1.6 Virology of Sars CoV-1
SARS-CoV-1 follows the replication strategy typical of the coronavirus subfamily. The primary human receptor of the virus is angiotensin-converting enzyme 2 (ACE2), first identified in 2003. Human SARS-CoV-1 appears to have had a complex history of recombination between ancestral coronaviruses that were hosted in several different animal groups. In order for recombination to happen at least two SARS-CoV-1 genomes must be present in the same host cell. Recombination may occur during genome replication when the RNA polymerase switches from one template to another (copy choice recombination).
1.7 Signs and symptoms of Sars CoV-1
SARS produces flu-like symptoms and may include fever, muscle pain, lethargy, cough, sore throat, and other nonspecific symptoms. The only symptom common to all patients appears to be a fever above 38 °C (100 °F). SARS may eventually lead to shortness of breath and pneumonia; either direct viral pneumonia or secondary bacterial pneumonia. The average incubation period for SARS is 4–6 days, although rarely it could be as short as 1 day or as long as 14 days.
1.8 Transmission of Sars CoV-1
The primary route of transmission for SARS-CoV is contact of the mucous membranes with respiratory droplets or fomites. While diarrhea is common in people with SARS, the fecal–oral route does not appear to be a common mode of transmission. The basic reproduction number of SARS-CoV, R0, ranges from 2 to 4 depending on different analyses. Control measures introduced in April 2003 reduced the R to 0.4.
1.9 Diagnosis of Sars CoV-1
SARS-CoV may be suspected in a patient who has: Any of the symptoms, including a fever of 38 °C (100 °F) or higher, and Either a history of: Contact (sexual or casual) with someone with a diagnosis of SARS within the last 10 days or Travel to any of the regions identified by the World Health Organization (WHO) as areas with recent local transmission of SARS. Clinical Criteria of Sars-Cov Diagnosis Early illness: equal to or more than 2 of the following: chills, rigors, myalgia, diarrhea, sore throat (self - reported or observed) Mild-to-Moderate illness: temperature of > 38 plus indications of lower respiratory tract infection (cough, dyspnea) Severe Illness: ≥1 of radiographic evidence, presence of ARDS, autopsy findings in late patients. For a case to be considered probable, a chest X-ray must be indicative for atypical pneumonia or acute respiratory distress syndrome. The WHO has added the category of ―laboratory confirmed SARS". Meaning, patients who would otherwise be considered "probable" and have tested positive for SARS based on one of the approved tests (ELISA, immunofluorescence or PCR) but have not yet shown chest X-ray findings pointing to SARS (e.g. ground glass opacities, patchy consolidations unilateral) The appearance of SARS-CoV in chest X-rays is not always uniform but generally appears as an abnormality with patchy infiltrates.
1.10 Prevention of Sars CoV-1
There is no vaccine for SARS, although immunologist Anthony Fauci mentioned that the CDC developed one and placed it in the US national stockpile. That vaccine, however, is a prototype and not field- ready as of March 2020.Clinical isolation and quarantine remain the most effective means to prevent the spread of SARS. Other preventive measures include: Hand-washing with soap and water, or use of alcohol-based hand sanitizer Disinfection of surfaces of fomites to remove viruses, Avoiding contact with bodily fluids, Washing the personal items of someone with SARS in hot, soapy water (eating utensils, dishes, bedding, etc.) Keeping children with symptoms home from school Simple hygiene measures Isolating oneself as much as possible to minimize the chances of transmission of the virus Many public health interventions were made to try to control the spread of the disease, which is mainly spread through respiratory droplets in the air, either inhaled or deposited on surfaces and subsequently transferred to a body’s mucous membranes. These interventions included earlier detection of the disease; isolation of people who are infected; droplet and contact precautions; and the use of personal protective equipment (PPE), including masks and isolation gowns. 2017 meta-analysis found that for medical professionals wearing N-95 masks could reduce the chances of getting sick up to 80% compared to no mask. A screening process was also put in place at airports to monitor air travel to and from affected countries. SARS-CoV is most infectious in severely ill patients, which usually occurs during the second week of illness. This delayed infectious period meant that quarantine was highly effective; people who were isolated before day five of their illness rarely transmitted the disease to others. Although no cases have been identified since 2004, as of 2017, the CDC was still working to make federal and local rapid-response guidelines and recommendations in the event of a reappearance of the virus.
1.11 Treatment of Sars CoV-1
As SARS is a viral disease, antibiotics do not have direct effect but may be used against bacterial secondary infection. Treatment of SARS is mainly supportive with antipyretics, supplemental oxygen and mechanical ventilation as needed. While Ribavirin is commonly used to treat SARS, there seems to have little to no effect on SARS-CoV, and no impact on patient's outcomes. There is currently no proven antiviral therapy. Tested substances, include ribavirin, lopinavir, ritonavir, type I interferon, that have thus far shown no conclusive contribution to the disease's course.
1.12 Vaccine of Sars CoV-1
As of 2020, there is no cure or protective vaccine for SARS that has been shown to be both safe and effective in humans. According to research papers published in 2005 and 2006, the identification and development of novel vaccines and medicines to treat SARS was a priority for governments and public health agencies around the world. In early 2004, an early clinical trial on volunteers was planned. A major researcher’s 2016 request, however, demonstrated that no field-ready SARS vaccine had been completed because likely market- driven priorities had ended funding.
1.13 Prognosis of Sars CoV-1
Several consequent reports from China on some recovered SARS patients showed severe long-time sequelae. The most typical diseases include, among other things, pulmonary fibrosis, osteoporosis, and femoral necrosis, which have led in some cases to the complete loss of working ability or even self-care ability of people who have recovered from SARS. As a result of quarantine procedures, some of the post- SARS patients have been documented as suffering from post-traumatic stress disorder (PTSD) and major depressive disorder.
1.14 Epidemiology of Sars CoV-1
SARS was a relatively rare disease; at the end of the epidemic in June 2003, the incidence was 8,422 cases with a case fatality rate (CFR) of 11%. The case fatality rate (CFR) ranges from 0% to 50% depending on the age group of the patient. Patients under 24 were least likely to die (less than 1%); those 65 and older were most likely to die (over 55%). As with MERS and COVID-19, SARS resulted in significantly more deaths of males than females. Probable cases of SARS by country or region, 1 November 2002 – 31 July 2003. After 11 July 2003, 325 Taiwanese cases were 'discarded'. Laboratory information was insufficient or incomplete for 135 of the discarded cases; 101 of these patients died. The viral outbreak can be genetically traced to a colony of cave-dwelling horseshoe bats in China's Yunnan. The SARS epidemic appears to have started in Guangdong, China, in November 2002 WHERE the first case was reported that same month. The patient, a farmer from S hunde, F oshan, Guangdong, was treated in the First People's Hospital of Foshan. The patient died soon after, and no definite diagnosis was made on his cause of death. Despite taking some action to control it, Chinese government officials did not inform the World Health Organization of the outbreak until February 2003. This lack of openness caused delays in efforts to control the epidemic, resulting in criticism of the People's Republic of China from the international community. China officially apologized for early slowness in dealing with the SARS epidemic. The outbreak first came to the attention of the international medical community on 27 November 2002, when Canada's Global Public Health Intelligence Network (GPHIN), an electronic warning system that is part of the World Health Organization's Global Outbreak Alert and Response Network (GOARN), picked up reports of a "flu outbreak" in China through Internet media monitoring and analysis and sent them to the WHO. While GPHIN's capability had recently been upgraded to enable Arabic, Chinese, English, French, Russian, and Spanish translation, the system was limited to English or French in presenting this information. Thus, while the first reports of an unusual outbreak were in Chinese, an English report was not generated until 21 January 2003. The first super-spreader was admitted to the Sun Yat-sen. Memorial Hospital in Guangzhou on 31
January, which soon spread the disease to nearby hospitals. Subsequent to this, the WHO requested information from Chinese authorities on 5 and 11 December. Despite the successes of the network in previous outbreaks of diseases, it did not receive intelligence until the media reports from China several months after the outbreak of SARS. Along with the second alert, WHO released the name, definition, as well as an activation of a coordinated global outbreak response network that brought sensitive attention and containment procedures. By the time the WHO took action, over 500 deaths and an additional 2,000 cases had already occurred worldwide.
In early April 2003, after a prominent physician, J iang Yanyong, pushed to report the danger to China, there appeared to be a change in official policy when SARS began to receive a much greater prominence in the official media. Some have directly attributed this to the death of an American teacher, James Earl Salisbury, in Hong Kong. It was around this same time that Jiang Yanyong made accusations regarding the undercounting of cases in Beijing military hospitals. After intense pressure, Chinese officials allowed international officials to investigate the situation there. This revealed problems plaguing the aging mainland Chinese healthcare system, including increasing decentralization, red tape, and inadequate communication. Many healthcare workers in the affected nations risked and lost their lives by treating patients, and trying to contain the infection before ways to prevent infection were known.
Table
|
Country or region |
Cases |
Deaths |
Fatality (%) |
|
|
5,327 |
349 |
6.6 |
|
Hong Kong |
1,755 |
299 |
17.0 |
|
|
346 |
73[34][35] |
21.1 |
|
|
251 |
43 |
17.1 |
|
Singapore |
238 |
33 |
13.9 |
|
Vietnam |
63 |
5 |
7.9 |
|
|
27 |
0 |
0 |
|
|
14 |
2 |
14.3 |
|
|
9 |
2 |
22.2 |
|
Germany |
9 |
0 |
0 |
|
|
9 |
0 |
0 |
|
France |
7 |
1 |
14.3 |
|
|
6 |
0 |
0 |
|
|
5 |
2 |
40. |
|
|
5 |
0 |
0 |
|
|
4 |
0 |
0 |
|
Italy |
4 |
0 |
0 |
|
Brazil |
3 |
0 |
0 |
|
India |
3 |
0 |
0 |
|
|
3 |
0 |
0 |
|
|
2 |
0 |
0 |
|
|
1 |
1 |
100.0 |
|
Colombia |
1 |
0 |
0 |
|
|
1 |
0 |
0 |
|
|
1 |
0 |
0 |
|
|
1 |
0 |
0 |
|
|
1 |
0 |
0 |
|
Romania |
1 |
0 |
0 |
|
|
1 |
0 |
0 |
|
Spain |
1 |
0 |
0 |
|
|
1 |
0 |
0 |
|
Total excluding China[a] |
2,769 |
454 |
16.4 |
1.15 Spread to other regions of Sars CoV-1
The epidemic reached the public spotlight in February 2003, when an American businessman traveling from China, Johnny Chen, became afflicted with pneumonia-like symptoms while on a flight to Singapore. The plane stopped in Hanoi, Vietnam, where the victim died in H anoi French Hospital. Several of the medical staff who treated him soon developed the same disease despite basic hospital procedures. Italian doctor Carlo Urbani identified the threat and communicated it to WHO and the Vietnamese government; he later succumbed to the disease. The severity of the symptoms and the infection among hospital staff alarmed global health authorities, who were fearful of another emergent pneumonia epidemic. On 12 March 2003, the WHO issued a global alert, followed by a health alert by the United States Centers for Disease Control and Prevention (CDC). Local transmission of SARS took place in Toronto, Ottawa, San Francisco, Ulaanbaatar, M anila, Singapore, Taiwan, Hanoi and Hong Kong whereas within China it spread to Guangdong, Jilin, Hebei, Hubei, Shaanxi, Jiangsu, Shanxi, Tianjin, and Inner Mongolia.
The World Health Organization declared severe acute respiratory syndrome contained on 5 July 2003. In the following years, four SARS cases were reported in China between December 2003 and January 2004. There were also three separate laboratory accidents that resulted in infection. In one of these cases, an ill lab worker spread the virus to several other people. Study of live SARS specimens requires a biosafety level 3 (BSL-3) facility; some studies of inactivated SARS specimens can be done at biosafety level 2 facilities.
Figure
syndrome coronavirus 2 (SARS- COV-2) COVID-19:
Severe acute respiratory syndrome coronavirus 2 (SARS- COV-2) is the strain of coronavirus that causes coronavirus disease 2019 (COVID-19), the respiratory illness responsible for the COVID-19 pandemic. Colloquially known as simply the name, 2019 novel coronavirus (2019-NCOV) and has also been called human coronavirus 2019 (HCoV-19 or hCoV-19). The World Health Organization declared the outbreak a Public Health Emergency of International Concern on 30 January 2020, and a pandemic on 11 March 2020. SARS-COV-2 is a Baltimore class IV positive-sense single- stranded RNA virus that is contagious in humans. As described by the U.S. National Institutes of Health, it is the successor to SARS-COV-1, the strain that caused the 2002– 2004 SARS outbreak. Taxonomically, SARS-COV-2 is a strain of severe acute respiratory syndrome-related coronavirus (SARSr-CoV). It is believed to have zoonotic origins and has close genetic similarity to bat coronaviruses, suggesting it emerged from a bat-borne virus. There is no evidence yet to link an intermediate animal reservoir, such as a pangolin, to its introduction to humans. The virus shows little genetic diversity, indicating that the spillover event introducing SARS-COV-2 to humans is likely to have occurred in late 2019. Epidemiological studies estimate each infection results in 1.4 to 1.9 new ones when no members of the community are immune and no preventive measures taken. The virus primarily spreads between people through close contact and via respiratory droplets produced from coughs or sneezes. It mainly enters human cells by binding to the receptor angiotensin converting enzyme 2 (ACE2).
Figure
1.17 Terminology of (SARS- COV-2) COVID-19
During the initial outbreak in Wuhan, China, various names were used for the virus; some names used by different sources included the "coronavirus" or "Wuhan coronavirus‖. In January 2020, the World Health Organization recommended "2019 novel coronavirus" (2019- NCOV)as the provisional name for the virus. This was in accordance with WHO's 2015 guidance against using geographical locations, animal species, or groups of people in disease and virus names. On 11 February 2020, the International Committee on Taxonomy of Viruses adopted the official name "severe acute respiratory syndrome coronavirus 2" (SARS-COV-2). To avoid confusion with the disease SARS, the WHO sometimes refers to SARS-CoV-2 as "the COVID-19 virus" in public health communications and the name HCOV- 19 was included in some research articles. The general public often call both SARS-COV-2 and the disease it causes "coronavirus". U.S. President Donald Trump referred to the virus as the ―Chinese virus‖ in tweets, interviews, and White House press briefings.
1.18 Virology Infection and transmission of (SARS- COV-2) COVID-19
Human-to-human transmission of SARS-COV-2 WAS confirmed on 20 January 2020, during the COVID-19 pandemic. Transmission was initially assumed to occur primarily via respiratory droplets from coughs and sneezes within a range of about 1.8 meters (6 ft.). Laser light scattering experiments suggest speaking as an additional mode of transmission. Other studies have suggested that the virus may be airborne as well. Indirect contact via contaminated surfaces is another possible cause of infection. Preliminary research indicates that the virus may remain viable on plastic (polypropylene) and stainless steel (AISI 304) for up to three days, but does not survive on cardboard for more than one day or on copper for more than four hours; the virus is inactivated by soap, which destabilizes its lipid bilayer. Viral RNA has also been found in stool samples and semen from infected individuals.
The degree to which the virus is infectious during the incubation period is uncertain, but research has indicated that the pharynx reaches peak viral load approximately four days after infection or the first week of symptoms, and declines after. On 1 February 2020, the World Health Organization (WHO) indicated that "transmission from asymptomatic cases is likely not a major driver of transmission". However, an epidemiological model of the beginning of the outbreak in China suggested that "pre-symptomatic shedding may be typical among documented infections" and that subclinical infections may have been the source of a majority of infections. That may explain how out of 217 on board a cruise liner that docked at Montevideo, only 24 of 128 who tested positive for viral RNA showed symptoms. Similarly, a study of ninety-four patients hospitalized in January and February 2020 estimated patients shed the greatest amount of virus two to three days before symptoms appear and that "a substantial proportion of transmission probably occurred before first symptoms in the index case‖. There is some evidence of human-to-animal transmission of SARS-COV-2, including examples in felids. Some institutions have advised those infected with SARS-COV-2 to restrict contact with animals. In July 2020, a preliminary scientific paper reported that a major genetic risk factor of the COVID-19 virus was inherited from archaic N review. Neanderthals ~60,000 years ago. The paper has yet to undergo peer
Figure

Potential transmission routes for SARS-CoV-2.
1.19 Reservoir and zoonotic origin of (SARS- COV-2) COVID-19
The first known infections from the SARS-COV-2 strain were discovered in Wuhan, China. The original source of viral transmission to humans remains unclear, as does whether the strain became pathogenic before or after the spillover event. Because many of the first individuals found to be infected by the virus were workers at the Huanan Seafood Market, it has been suggested that the strain might have originated from the market. However, other research indicates that visitors may have introduced the virus to the market, which then facilitated rapid expansion of the infections. A phylogenetic network analysis of 160 early coronavirus genomes sampled from December 2019 to February 2020 revealed that the virus type most closely related to the bat coronavirus was most abundant in Guangdong, China, and designated type "A". The predominant type among samples from Wuhan, "B", is more distantly related to the bat coronavirus than the ancestral type "A".Research into the natural reservoir of the virus strain that caused the 2 002–2004 SARS outbreak has resulted in the discovery of many SARS-like bat coronaviruses, most originating in the Rhinolophus genus of horseshoe bats. Phylogenetic analysis indicates that samples taken from Rhinolophus sinicus show a resemblance of 80% to SARS-COV-2. Phylogenetic analysis also indicates that a virus from Rhinolophus affine, collected in Yunnan province and designated RATG13, has a 96% resemblance to SARS-COV-2. Bats were initially considered to be the most likely natural reservoir of SARS-COV-2, which means that they harbour the virus for long periods of time with no pathogenic effects. Regarding the animal source of infection into humans, the differences between the bat coronavirus sampled at the time and SARS-COV-2 suggested that humans were infected via an intermediate host. Arinjay Banerjee, a virologist at McMaster University, notes that "the SARS virus shared 99.8% of its genome with a civet coronavirus, which is why civets were considered the source. ―Although studies had suggested some likely candidates, the number and identities of intermediate hosts remains uncertain. Nearly half of the strain's genome had a phylogenetic lineage distinct from known relatives. A phylogenetic study published in 2020 indicates that pangolins are a reservoir host of SARS-COV-2-LIKE coronaviruses. However, there is no direct evidence to link pangolins as an intermediate host of SARS-COV-2 at this moment. While there is scientific consensus that bats are the ultimate source of coronaviruses, it is hypothesized that a SARS-COV-2-LIKe coronavirus originated in pangolins, jumped back to bats, and then jumped to humans, resulting in SARS-COV-2. Based on whole genome sequence similarity, a pangolin coronavirus candidate strain was found to be less similar than RATG13, but more similar than other bat coronaviruses to SARS-COV-2. Therefore, based on maximum parsimony, a specific population of bats is more likely to have directly transmitted SARS-COV-2 to humans than a pangolin, while an evolutionary ancestor to bats was the source of general coronaviruses.
A metagenomics study published in 2019 had previously revealed that SARS-CoV, the strain of the virus that causes SARS, was the most widely distributed coronavirus among a sample of Sunda pangolins. On 7 February 2020, South China Agricultural University in Guangzhou announced that researchers discovered a pangolin sample with a particular coronavirus – a single nucleic acid sequence of the virus was "99% similar" to that of a protein-coding RNA of SARS-COV-2.The authors state that "the receptor-binding domain of the S protein [that binds to the cell surface receptor during infection] of the newly discovered Pangolin-CoV is virtually identical to that of 2019-NCOV, with one amino acid difference." Microbiologists and geneticists in Texas have independently found evidence of assortment in coronaviruses suggesting involvement of pangolins in the origin of SARS-COV- 2.The majority of the viral RNA is related to a variation of bat coronaviruses. The spike protein appears to be a notable exception, however, possibly acquired through a more recent recombination event with a pangolin coronavirus. Structural analysis of the receptor binding domain (RBD) and human angiotensin-converting enzyme 2 (ACE2) complex revealed key mutations on the RBD, such as F486 and N501, which form contacts with ACE2. These residues are found in the pangolin coronavirus.
Pangolins are protected under Chinese law, but their poaching and trading for use in traditional Chinese medicine remains common in the black market. Deforestation, wildlife farming and trade in unsanitary conditions increases the risk of new zoonotic diseases, biodiversity experts have warned. It is unlikely that SARS-COV-2 WAS genetically engineered. According to computational simulations on protein folding, the RBD of the spike protein of SARS-COV-2 should have unremarkable binding affinity. In actuality, however, it has very efficient binding to the human ACE2 receptor. To expose the RBD for fusion, furan proteases must first cleave the S protein. Furin proteases are abundant in the respiratory tract and lung epithelial cells. Additionally, the backbone of the virus does not resemble any previously described in scientific literature used for genetic modification. The possibility that the virus could have gained the necessary an adaptations through cell culture in a laboratory setting is challenged by scientists who assert that "the generation of the predicted O-linked glycan’s... suggest the involvement of an immune system."
1.20 Phylogenetic and taxonomy of (SARS- COV-2) COVID-19
SARS-COV-2 belongs to the broad family of viruses known as coronaviruses. It is a positive- sense single-stranded RNA (+ssRNA) virus, with a single linear RNA segment. Other coronaviruses are capable of causing illnesses ranging from the common cold to more severe diseases such as Middle East respiratory syndrome (MERS, fatality rate ~34%). It is the seventh known coronavirus to infect people, after 229E, NL63, OC43, HKU1, MERS-CoV, and the original SARS-CoV. Like the SARS-related coronavirus strain implicated in the 2003 SARS outbreak, SARS-COV-2 is a member of the subgenus Sarbecovirus (beta-CoV lineage B).Its RNA sequence is approximately 30,000 bases in length.SARS-COV-2 is unique among known beta coronaviruses in its incorporation of a polybasic cleavage site, a characteristic known to increase Pathogenicity and transmissibility in other viruses. With a sufficient number of sequenced genomes, it is possible to reconstruct a phylogenetic tree of the mutation
history of a family of viruses. By 12 January 2020, five genomes of SARS- COV-2 had been isolated from Wuhan and reported by the Chinese Center for Disease Control and Prevention (CCDC) and other institutions; the number of genomes increased to 42 by 30 January 2020. A phylogenetic analysis of those samples showed they were "highly related with at most seven mutations relative to a common ancestor", implying that the first human infection occurred in November or December 2019.As of 7 May 2020, 4,690 SARS- COV-2 genomes sampled on six continents were publicly available. On 11 February 2020, the International Committee on Taxonomy of Viruses announced that according to existing rules that compute hierarchical relationships among coronaviruses on the basis of five conserved sequences of nucleic acids, the differences between what was then called 2019- NCoV and the virus strain from the 2003 SARS outbreak were insufficient to make them separate viral species. Therefore, they identified 2019-NCOV as a strain of severe acute respiratory syndrome-related coronavirus. In July 2020, scientists report that a more infectious SARS-COV-2 variant with spike protein variant G614 has replaced D614 as the dominant form in the pandemic.
1.21 Structural biology of (SARS- COV-2) COVID-19
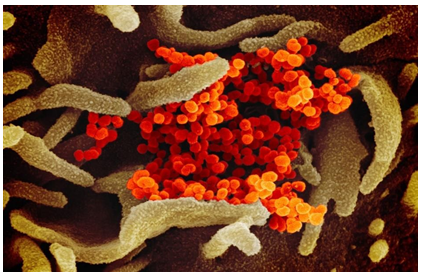
Each SARS-COV-2 virion is 50–200 nanometers in diameter. Like other coronaviruses, SARS-CoV-2 has four structural proteins, known as the S (spike), E (envelope), M (membrane), and N (nucleocapsid) proteins; the N protein holds the RNA genome, and the S, E, and M proteins together create the viral envelope. The spike protein, which has been imaged at the atomic level using cryogenic electron microscopy, is the protein responsible for allowing the virus to attach to and fuse with the membrane of a host cell; specifically, its S1 subunit catalyzes attachment, the S2 subunit fusion. Protein modeling experiments on the spike protein of the virus soon suggested that SARS-COV-2 has sufficient affinity to the receptor angiotensin converting enzyme 2 (ACE2) on human cells to use them as a mechanism of cell entry. By 22 January 2020, a group in China working with the full virus genome and a group in the United States using reverse genetics methods independently and experimentally demonstrated that ACE2 could act as the receptor for SARS-COV-2.Studies have shown that SARS-COV-2 has a higher affinity to human ACE2 than the original SARS virus strain. SARS-COV-2 may also use basigin to assist in cell entry. Initial spike protein priming by transmembrane protease, serine 2 (TMPRSS2) is essential for entry of SARS-COV-2. After a SARS-COV-2 virion attaches to a target cell, the cell's protease TMPRSS2 cuts open the spike protein of the virus, exposing a fusion peptide in the S2 subunit, and the host receptor ACE2.After fusion, an endosome forms around the virion, separating it from the rest of the host cell. The virion escapes when the pH of the endosome drops or when cathepsin, a host cysteine protease, cleaves it. The virion then releases RNA into the cell and forces the cell to produce and disseminate copies of the virus, which infect more cells.SARS- COV-2 produces at least three virulence factors that promote shedding of new virions from host cells and inhibit immune response. Whether they include downregulation of ACE2, as seen in similar coronaviruses, remains under investigation (as of May 2020).Digitally colorized scanning electron micrographs of SARS-CoV-2 virions (yellow) emerging from human cells cultured in a laboratory
1.22 Epidemiology of (SARS- COV-2) COVID-19
Based on the low variability exhibited among known SARS-COV-2 genomic sequences, the strain is thought to have been detected by health authorities within weeks of its emergence among the human population in late 2019.The earliest case of infection currently known is dated back to 17 November 2019 or possibly 1 December 2019. The virus subsequently spread to all provinces of China and to more than 150 other countries in Asia, Europe, North America, South America, Africa, and Oceania. Human-to- human transmission of the virus has been confirmed in all these regions. On 30 January 2020, SARS-COV-2 WAS designated a Public Health Emergency of International Concern by the WHO, and on 11 March 2020 the WHO declared it a pandemic. The basic reproduction number ( ) of the virus has been estimated to be between 1.4 and 3.9.This means each infection from the virus is expected to result in 1.4 to 3.9 new infections when no members of the community are immune and no preventive measures are taken. The reproduction number may be higher in densely populated conditions such as those found on cruise ships. Many forms of preventive efforts may be employed in specific circumstances in order to reduce the propagation of the virus. There have been about 82,000 confirmed cases of infection in mainland China. While the proportion of infections that result in confirmed cases or progress to diagnosable disease remains unclear, one mathematical model estimated that 75,815 people were infected on 25 January 2020 in Wuhan alone, at a time when the number of confirmed cases worldwide was only 2,015. Before 24 February 2020, over 95% of all deaths from COVID-19 worldwide had occurred in Hubei province, where Wuhan is located. As of 29 August 2020, the percentage had decreased to 0.39%.As of 29 August 2020, there have been 24,637,544 total confirmed cases of SARS-COV-2 infection in the ongoing pandemic. The total number of deaths attributed to the virus is 835,045.Many recoveries from confirmed infections go unreported, but at least 16,107,859 people have recovered from confirmed infections.
1.23 Coronavirus pandemic of (SARS- COV-2) COVID-19
The 2019–20 coronavirus pandemic is an ongoing pandemic of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). First identified in Wuhan, Hubei, China, in December 2019, the outbreak was recognized as a pandemic by the World Health Organization (WHO) on 11 March 2020.As of 18 March 2020, more than 204,000 cases of COVID-19 have been reported in over 160 countries and territories, with major outbreaks in mainland China, Europe, Iran, and South Korea. More than 8,200 people have died and over 82,000 have recovered. On 13 March, the WHO announced that Europe has become the new epicenter of the pandemic. On 31 December 2019, a cluster of pneumonia cases of unknown cause was reported by health authorities in Wuhan, the capital of Hubei province, China, and an investigation was launched in early January 2020. These cases mostly had links to the Huanan Seafood Wholesale Market, which also sold live animals; consequently, the virus is thought to have a zoonotic origin. The virus that caused the outbreak is known as SARS-CoV-2, a new virus closely related to bat coronaviruses, pangolin coronaviruses and SARS-CoV. It is believed that the virus possibly originated in horseshoe bats (genus Rhinolophus).The earliest person with symptoms was traced back to 1 December 2019, someone who did not have connections with the later cluster linked to the wet market. Of the early cluster of cases reported in December 2019, two-thirds were found to have a link with the market. On 14 March 2020, an unverified report from the South China Morning Post said that a 55year-old from Hubei province could have been the first person who contracted the disease on 17 November. Asia Pakistan etc. spread. Effects of the pandemic include social and economic instability, the postponement or cancellation of sporting and cultural events, the suspension of in-person religious services, xenophobia and racism against Chinese, East and Southeast Asian people as well as the online spread of misinformation and conspiracy theories about the virus.
1.24 WHO Role in (SARS- COV-2) COVID-19:
On March 11, 2020, the World Health Organization (WHO) had declared COVID-19 a pandemic because of alarming levels of its spread, severity and inaction. COVID-19 is caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), which is sufficiently genetically divergent from the closely related Severe Acute Respiratory Syndrome Coronavirus (SARS- CoV), to be considered a new human-infecting beta coronavirus. It mainly affects the respiratory tract and the illness ranges in severity from asymptomatic or mild to severe or critical disease. Although the current estimate of the case fatality rate of COVID-19 is < 5%, up to 15–18% of patients may become severe or critically ill, some of them requiring ICU care and mechanical ventilation On 26 February 2020, the WHO reported that, as new cases reportedly dropped in China but suddenly increased in Italy, Iran, and South Korea, the number of new cases outside China had exceeded the number of new cases in China for the first time. There may be substantial underreporting of cases, particularly among those with milder symptoms. Reported numbers may also reflect local decisions on whom and when to test. As an example, on 13 March 2020, the UK reported 798 confirmed cases, but health officials estimated the actual number of people infected was probably between 5,000 and 10,000. Since December 2019, a new strain of coronavirus named 2019 novel coronavirus (2019-nCoV) has been discovered in Wuhan. The prevalence of diabetes mellitus, which is a great public health issue leading to immunity inhibition and an increased incidence of infections, has been increasing over the past ten years. The aim of this research was to systematically assess the prevalence of diabetes mellitus among 2019-nCoV Since COVID-19 is a new disease, knowledge about this disease is still incomplete and evolving. Many case-control studies have shown that patients of COVID-19, who have underlying diabetes mellitus, develop a severe clinical course, and also have increased mortality. However, most of these studies have small sample size, and the data in them are heterogeneous and conflicting. In addition, the data on prevalence of diabetes in patients with COVID-19 is also not clear. Hence, this meta-analysis was conducted with the primary objective of exploring the relationship between underlying diabetes and severity and mortality of COVID-19 disease; and with the secondary objective of determining the prevalence of diabetes in patients with COVID-19.
Figure WHO Mortality rate of (SARS- COV-2)
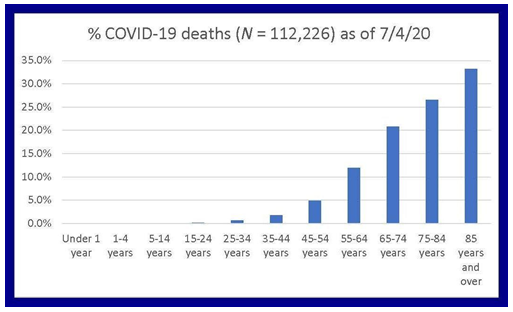
1.25 Mortality rate of (SARS- COV-2) COVID-19:
Among those who died from the disease, the time from development of symptoms to death was between 6 and 41 days, with a median of 14 days. As of 18 March 2020, more than 8,200 deaths have been attributed to COVID-19. According to China's NHC, most of those who died were elderly – about 80% of deaths were in those over 60, and 75% had pre-existing health conditions including cardiovascular diseases and diabetes. The first confirmed death was on 9 January 2020 in Wuhan. The first death outside China occurred on 1 February in the Philippines, and the first death outside Asia was in France. By 28 February, outside mainland China, more than a dozen deaths were recorded in each of Iran, South Korea and Italy. By 13 March, over 40 countries and territories had reported deaths, on every continent Except Antarctica.
Figure
1.26 Prevention and Treatment of (SARS- COV-2) COVID-19:
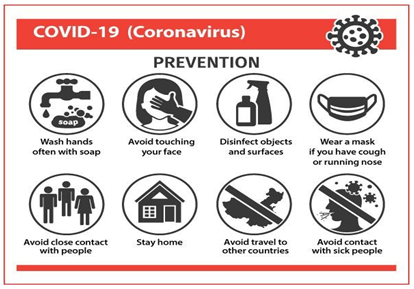
Strategies for preventing transmission of the disease include overall good personal hygiene, hand washing, avoiding touching the eyes, nose or mouth with unwashed hands, coughing/sneezing into a tissue and putting the tissue directly into a dustbin. Those who may already have the infection have been advised to wear a surgical mask in public. Social distancing measures are also recommended to prevent transmission. Many governments have restricted or advised against all nonessential travel to and from countries and areas affected by the outbreak. However, the virus has reached the stage of community spread in large parts of the world. This means that the virus is spreading within communities whose members have not travelled to areas with widespread transmission. Health care providers taking care of someone who may be infected are recommended to use standard precautions, contact precautions and airborne precautions with eye protection. Contact tracing is an important method for health authorities to determine the source of an infection and to prevent further transmission. Misconceptions are circulating about how to prevent infection, for example: rinsing the nose and gargling with mouthwash are not effective. As of 13 March 2020, there is no COVID-19 vaccine though a number of organizations are working to develop one. China has banned the trading and consumption of wild animals. Ways of prevention and safety precautions are Hand wash, social distancing, respiratory hygiene’s, self-isolation, management. Evacuations of foreign citizens, travel restrictions, international aids grants funds, WHO measures for safety, Efforts to prevent spread have included travel restrictions, quarantines, curfews, event postponements and cancellations, and facility closures.
1.27 Impacts of coronavirus of (SARS- COV-2) COVID-19
Social, economic, political, environmental, socio-economical, cultural and religious, education, societal. The outbreak of coronavirus disease (COVID-19) has severely affected the global and world economy. Major victims of the COVID-19 outbreak are micro, small, and medium-sized enterprises (MSMEs). This article aims to assess the impact of COVID-19 outbreak on these businesses and provide policy recommendations to help MSMEs in reducing business losses and survive through the crisis.
Conclusion
Suggestions are made on the possible pathophysiological mechanisms of the relationship between diabetes and COVID-19, and its management. No definite conclusions can be made based on current limited evidence. Further research regarding this relationship and its clinical management is warranted. Patients with diabetes are considered to be at higher risk for severe illness. They are more likely to need intensive care if they develop COVID-19 compared with patients who do not have diabetes and have a higher case fatality rate10, 19. Diabetes may not increase the risk of COVID-19 infection but it can lead to enhanced disease severity. Preliminary findings from the United States14 suggest that persons with underlying health conditions or other recognized risk factors for severe outcomes from respiratory infections appear to be at a higher risk for severe disease from COVID19 than are persons without these conditions. The most commonly reported conditions were diabetes mellitus, chronic lung disease and cardiovascular disease. The Centre for Evidence-Based Medicine5 states that there is little evidence on how people with diabetes can reduce their risk of COVID-19 infection beyond following general infection control guidance. Significant disruptions to routine care may also contribute to poorer outcomes during and following the pandemic. Hyperglycemia should not be overlooked, but adequately treated to improve the outcomes of COVID-19 patients with our without diabetes25. Both the HPSC1 and WHO3 highlight evidence suggesting there are two groups of people at a higher risk of acquiring a more severe disease; older people and those with an underlying medical condition such as diabetes. Clinical guidance from the CDC4 also highlights risk factors for severe illness and reports that fatality is higher for patients with diabetes. Diabetes as a distinctive comorbidity is associated with more severe disease, acute respiratory distress syndrome and increased mortality12. In a nationwide analysis on comorbidity and its impact on patients in China23, Guan et al found that the most prevalent comorbidity was hypertension followed by diabetes. The study concludes that patients with any comorbidity yielded poorer clinical outcomes than those without, and that a greater number of comorbidities also correlated with poorer clinical outcomes. Discussing two earlier CoV infections SARS and MERS Bloom garden et al34 report that regardless of the potential for the spread of COVID-19, as with influenza-reported mortality diabetes is an important risk factor for adverse outcome. Diabetes should be considered a risk factor and more intensive attention should be paid to patients with diabetes, in case of rapid deterioration.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgements
The authors would like to thank you the University of the Punjab, Lahore, Punjab, Family Physician of Pakistan to Hospitals and Laboratories from Lahore and Family on for getting data assisting and help and support. All authors reviewed and approved the final version of the manuscript.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org
 China[a]
China[a] Taiwan[b]
Taiwan[b] Canada
Canada United States
United States Philippines
Philippines Thailand
Thailand Mongolia
Mongolia Australia
Australia Malaysia
Malaysia Sweden
Sweden United Kingdom
United Kingdom South Korea
South Korea Indonesia
Indonesia South Africa
South Africa Kuwait
Kuwait Ireland
Ireland Macao
Macao New Zealand
New Zealand Russia
Russia Switzerland
Switzerland