Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Jochanan E. Naschitz
The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel
*Corresponding author: Jochanan E. Naschitz, The Ruth and Bruce Rappaport Faculty of Medicine, Technion, Israel Institute of Technology, Haifa, Israel.
Received: February 03, 2021
Accepted: February 21, 2021
Published: March 03, 2021
Citation: Jochanan E. Naschitz. “Herpes Labialis, Herpetic Whitlow and Genital Herpes by Autoinoculation”. Clinical Case Reports and Clinical Study, 3(1) ; DOI: 10.61148/2766-8614/JCCRCS/029
Copyright: © 2021 Jochanan E. Naschitz. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
A 10-year-old boy in good general health presented with a 5-day history painful burning and itching of fingertips. Physical examination revealed two lesions on the distal phalanx of the right thumb: one ruptured vesicle 3 mm in diameter and a round superficial dermal suffusion 8 mm in diameter on the fingertip
Introduction
A 10-year-old boy in good general health presented with a 5-day history painful burning and itching of fingertips. Physical examination revealed two lesions on the distal phalanx of the right thumb: one ruptured vesicle 3 mm in diameter and a round superficial dermal suffusion 8 mm in diameter on the fingertip. A similar lesion on the left index finger extended below the fingernail (Figure 1). Two weeks earlier he had a recurrence of herpes labialis (Figure 2), from which he was suffering several times since age 3. Neither recurrence of herpes labialis nor the eruption on the fingers was associated with general symptoms. He was given a clinical diagnosis of herpetic whitlow. A 7-day course of oral acyclovir 5% ointment was applied to the involved areas of the fingers. Within 3 days the improved and within another week the eruption disappeared. Six months later two herpetic lesions appeared on the penile shaft in the absence of fever. Acyclovir treatment, 400 mg orally 3 times per day for 7 days, provided quick remission.

Figure 1: Herpetic whitlow, vesicle and suffusions.
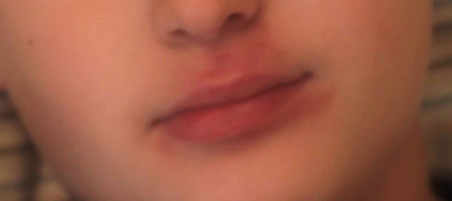
Figure 2: Herpes labialis in remission. The herpetic eruption had involved the vermilion border of the lips and the adjacent skin. Vesicles and crusts are no longer visible.
Herpetic whitlow is caused by herpes simplex viruses type 1 or 2 [1]. In children less than 10 years of age, 80–90% of herpetic infections are caused by herpes simplex vurus-1 [2]. Primary infection occurs by direct contact transmission from an infected person through broken skin, or autogenously transmitted from one site to the other. One or more painful vesicles appear around the nail, than dry and crust. The natural course of the infection in the immunocompetent patient is spontaneous resolution in 2 to 4 weeks (3,4). Herpetic whitlow is a clinical diagnosis [1-6]. The diagnosis is important given its close similarity on presentation to paronychia and its different treatment.
Genital herpes simplex virus infection is the leading cause of genital ulcer disease, efficiently transmitted through intimate genital tract contact and causes persistent infection that cannot be eliminated [7]. In young children autoinoculation was a frequent route of transmission to the genitalia [8]. Clinicians should be aware of the weakness of the evidence on the likelihood of sexual transmission of genital herpes in prepubertal children [9].
Antiviral agents are effective in controlling clinical episodes, but do not eradicate infection, which remains latent for the life of a patient. For treating herpetic whitlow, the role of antiviral agents (e.g. acyclovir) is still debated, treatment should be considered in immunocompromised patients, yet treatment is clearly indicated in symptomatic genital herpes [2,7]. Acyclovir selectively inhibits the viral DNA polymerase and is incorporated in the growing viral DNA chain, causing chain termination. The drug becomes active only in virus-infected cells, which contributes to its excellent safety profile [10].
Autoinoculation from herpes labialis to the fingers caused herpetic whitlow and to the penile shaft caused genital herpes. Awareness to potential autoinoculation permits straightforward diagnosis.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org