Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Takaki Shimura1*, Eriko Okuyama2, Atsuko Suzuki1 and Hironori Ohsugi3
1BME Research Lab. Sosei Ltd., Japan
2Hamamatsu Human Research Lab. Ltd., Japan
3Josai International University, Japan
*Corresponding Author: Takaki Shimura, BME Research Lab. Sosei Ltd., Japan.
Received: December 18, 2022
Accepted: December 22, 2022
Published: December 26, 2022
Citation: Takaki Shimura, Eriko Okuyama, Atsuko Suzuki1 and Hironori Ohsugi (2022) “Regional disparities in diagnostic results using CKPT (Japanese version of CWPT)”, Clinical Case Reports and Clinical Study, 1(8); DOI: http;//doi.org/12.2022/1.155.
Copyright: © 2022 Takaki Shimura. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
Objective: CKPT, Japanese version of CWPT (Color words Pick-out Test), which is a neuropsychological test that detects slight declines in brain function before dementia, have been accumulated since 2006 in various areas in Japan. The purpose of this analysis is to examine the regional disparities in diagnostic results using CKPT.
Methods: The tests were conducted in four areas: suburbs of large cities, urban areas of medium-sized cities, small cities, and rural / fishing village areas. The test paper, test environment such as lighting and room temperature, level of testers, ratio of test supervisors, test execution tools, etc. were standardized. Subjects were people who thought they were without dementia. We extracted the group who needs clinical treatment under a certain standard and get clinical treatment ratio named CTR. The ratio is calculated in each area and the regional disparities are examined using that ratio.
Results: A total of 1325 subjects were included, including 82 in suburbs of large cities, 256 in urban areas of middle cities, 559 in small cities, and 428 in rural / fishing village areas. No significant differences were found comparing CTR in each area with that of total area. No significant differences were also found between each area.
Conclusions: CTR of those who thought they did not have dementia increased with age. And the tendency seems almost the same in all area in Japan.
1. Background
Fig. 1 is a guideline for a diagnostic method for AD presented by Sperling et al1)., which shows that AD symptoms appear only after βA is deposited to a near-saturation level. After the failure of research on therapeutic drugs after the onset of dementia, the research paradigm has shifted to MCI2) and preclinical stages in recent years.Fig.2 illustrates the progression of degenerative types of dementia and the scope of application of CKPT. In the figure, the progression of cognitive impairment is shown from left to right, and the preclinical stage is an institution where cognitive impairment does not appear for 15 to 20 years when neurotransmission inhibitors continue to accumulate 1,3). Recently, research on dementia has shifted to the preclinical stage and MCI, and new needs arise for economical methods to determine the effects of both drug therapy and non-drug therapy. Molecular imaging methods such as PET which are available for diagnoses in the preclinical stage require exposure to radiation and high imaging costs, and do not meet this requirement. CSF4) also does not meet this requirement because of inversion. We have been focusing on neuropsychological tests that can be examined in groups.
Neuropsychological tests such as MMSE5) and CDR6), are tests applied after the onset of dementia. If they are applied before the onset of dementia, the histogram will be biased toward high scores as shown in Fig. 3(a), and classification cannot be performed. On the other hand, since CKPT histogram has a normal distribution, it is characteristic that it can be easily classified into classes using the mean and standard deviation in Fig.3(b).
CWPT was devised in 20037), and evidence has been established using CKPT8) which is the Japanese version of CWPT, and diagnostic criteria9) have been established using large-scale data. After that, the test was conducted on 1,325 subjects who said, "I don't have dementia" and "I don't want to fall into dementia." It has been founded that as the age increases, the rate of the people who are judged as abnormal increases10).
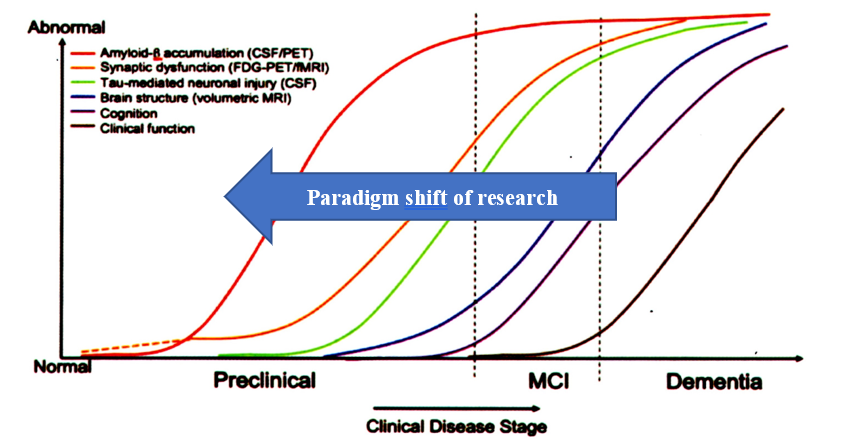
Fig.1 Diagnosis guideline by Sperling
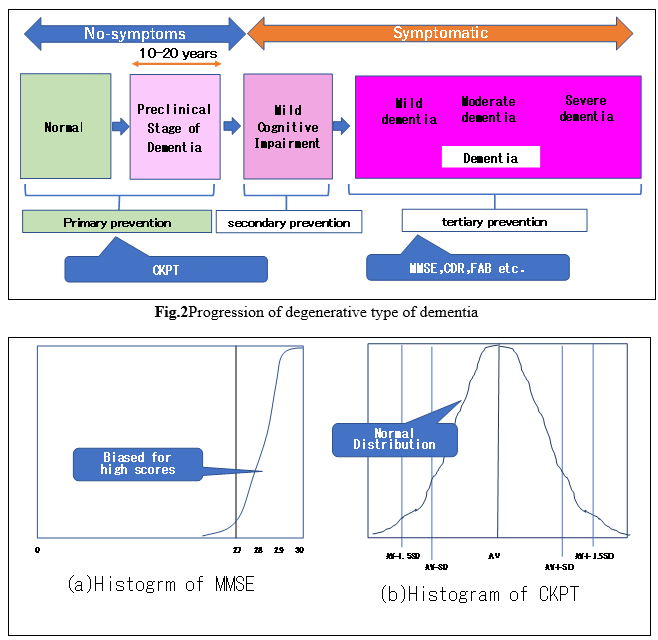
Fig.3 Comparison of histogram of MMSE and CKPT
2. Objective
Since 2006, data of Index1 obtained by CKPT, a neuropsychological test that detects slight declines in brain function before dementia, have been accumulated from various area. The purpose of this analysis is to examine the regional disparities in diagnostic results using CKPT.
3. Methods
3.1 Areas and environments of the screening
The screening tests were conducted in four areas: suburbs of a large city, urban areas of medium-sized cities, small cities, and rural / fishing village areas. The test paper, test environment such as lighting and room temperature, level of testers, ratio of test supervisors, test execution tools, etc. were standardized.
3.2 CKPT and Judgment
CKPT is a neuropsychological test that applies the Stroop effect11). In CKPT, Story including color words are shown first like Fig.4a. Subjects should read the story memorizing the episode of it, and simultaneously pick-out color words discerning the matching of meaning and printed color of them. If they are matched, the subject puts a circle on the colored word, and if they are not matched, puts a cross on the color word. After a certain period of time, the subjects stop the task of determining the color words of Story, and answer Questions (Fig.4b) regarding the episode memorized without seeing Story.
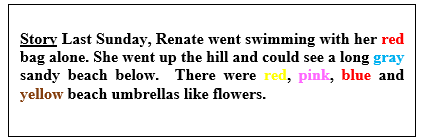
Fig.4a Sample of Story of CWPT
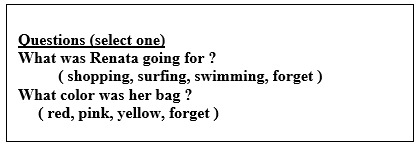
Fig.4b Sample of Questions
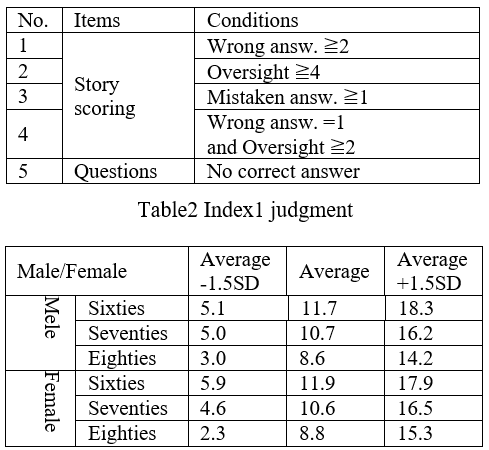
FIG. 5 shows a flow chart9) for judgment that a specialist should be consulted among subjects who do not think that I have dementia. Exclusion conditions in the figure are shown in Table 1, and criteria for Index1 are shown in Table 2. Those who ultimately require clinical treatment are either those selected by the exclusion condition or those with an Index1 Judgment of Average-1.5 SD or less. The ratio of those who need clinical treatment to all subjects was calculated and used for analysis as the Clinical Treatment Ratio (CTR).
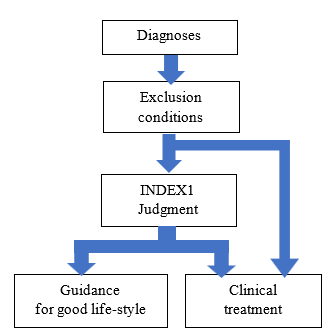
Fig.5 Flow chart of judgement using CKPT
Table1 Exclusion conditions
3.3 Analysis
We obtained CTR by each area and CTR in the whole, and examined whether there is a difference in CTR. First, the null hypothesis is that there is no difference in CTR, and the alternative hypothesis is that there is a difference in CTR. For the test, the Z score of the groups to be compared was obtained, and a two-sided test with a significance level of 5% was performed.
4. Results
Tables 3 shows the number of subjects, the number of people who is excluded by exclusion conditions, the number of people whose Index 1 value is less than the average -1.5 SD, and the CTR, by gender and age in each area. Table 4 represents the sum of all area.
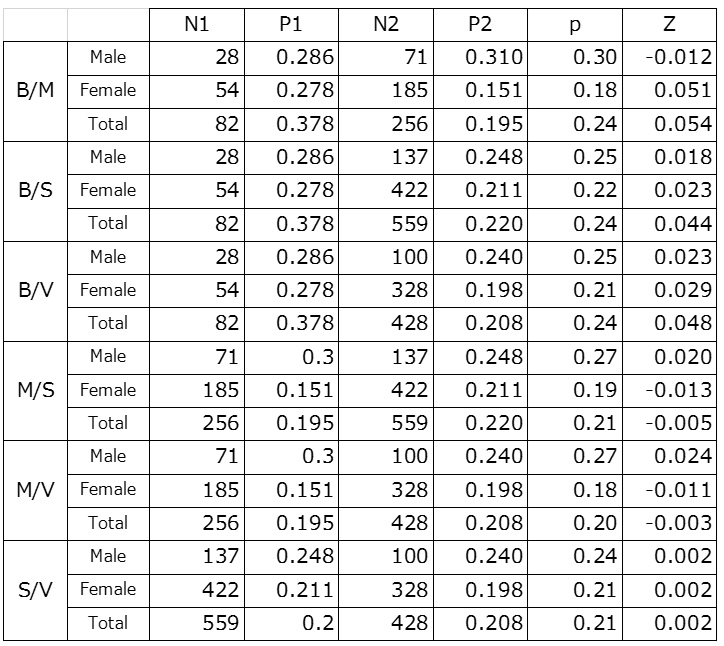
Z-score was obtained to test the difference in CTR in each area. First, in order to test the difference between the CTR value of the total area and the CTR value of each area, Z-scores were obtained and shown in Table 5. In the table, T/B, T/M, T/S, and T/V represent the test of the difference between total area and suburbs of a big city, urban area of middle cities, small cities, rural/fishing village, respectively. The significance level of 5% was tested.
Since Z-score of 5% is 1.96, it was found that there is no significant difference between CTR in all areas and one in total area. In addition, regarding the significant difference between regions, Z-score was obtained for all combinations and the same test was performed. The results are shown in Table5. Then it was found that there was no significant difference in all combinations.
Table5 Z score between total area and each area

Table6 Z score between each area
5. Considerations
Previous studies have shown that among the elderly who do not believe they have dementia10), there are those who require clinical treatment, and that the rate (CTR) increases with age. there is in this analysis
We investigated regional differences in CTR. As a result, it was found that there is no regional disparity in CTR in all regions of Japan. In particular, it was impressive that there was no significant difference in the test between large cities and farming villages/fishing villages.
Summery
So far, we have reported the results of retrospective studies using large-scale CKPT data. In the future, prospective studies using CKPT to determine the effects of rehabilitation for dementia prevention and the effects of preventive drugs for dementia are underway, and we would like to report on the results of these studies.
Finally, although CKPT is a Japanese version of CWPT, there is a tool for testing the English version12), so if you wont to introduce the technology, please contact tshimura@tuba.ocn.ne.jp.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org