Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Hèla Ben Jmaà 1*, Aiman Dammak 1, Majdi Gueldich 1, Faten Dhouib 2, Abir Bouassida 2, Mohamed Seddik1, Wael Jawadi 3, Hichem Denguir 2, Imed Frikha 1.
1Department of cardiovascular and thoracic surgery Habib Bourguiba Hospital Sfax Tunisia.
2Department of cardiology Mohamed Ben Sassi Hospital Gabes Tunisia.
3Depatment of anesthesiology Habib Bourguiba Hospital Sfax Tunisia.
*Corresponding author: Ben Jmaà Hèla, Department of cardiovascular and thoracic surgery Habib Bourguiba Hospital Sfax Tunisia.
Received: December 14, 2021
Accepted: December 23, 2021
Published: January 04, 2022
Citation: Ben Jmaà Hèla, Aiman Dammak, Majdi Gueldich, Faten Dhouib, Abir Bouassida, Mohamed Seddik, Wael Jawadi, Hichem Denguir, Imed Frikha “ Surgical Management Of Iatrogenic Aotic Dissection : A Case Illustration.” Clinical Case Reports and Clinical Study, 5(5) ; DOI : http;//doi.org/12.2022/1.121.
Copyright: © 2022 Ben Jmaà Hèla. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Iatrogenic coronary sinus of Valsalva dissection is a rare but fatal complication of percutaneous coronary intervention with a reported incidence of < 0.1%.
This dissection progressively extends to the ascending aorta. The appropriate therapeutic strategy of these lesions is still controversial.
We report the case of a 46-year-old man complaining of chest angina underwent emergent coronary angiogram and significant stenosis in the right coronary artery was discovered.
The procedure was complicated by iatrogenic dissection of the ostium of the coronary artery and the ascending aorta.
The patient underwent emergent surgery under cardio-pulmonary bypass between the femoral artery and the right atrium.
The intervention was a surgical repair of the intimal tear with conservation of the aorta.
The postoperative course was uneventful.
Introduction :
The prevalence of sophisticated instruments in the field of interventional cardiology in the past three decades has allowed these procedures to be performed more safely [1]. However, they may have some complications such as aortic dissection.
We report the case of a patient who underwent percuaneous right coronary artery angioplasty complicated by aortic dissection, and who was treated by surgery under cardio-pulmonary bypass.
Case report :
A 46-year-old man with history of blood hypertension and smoking presented with angina. His physical examination was unremarkable.
The electrocardiogram showed ST segment elevation, and echocardiogram was found to be normal.
The patient underwent coronary angiography which confirmed a stenosis of the right coronary artery. So, he completed by percutaneous coronary angioplasty. During procedure, and after removal of the stent balloon, the patient experienced sudden onset chest pain, while remaining hemodynamically stable.
Check angiography revealed retrograde dissection from the right coronary artery to the aorta with intra-mural hematoma (figure 1).
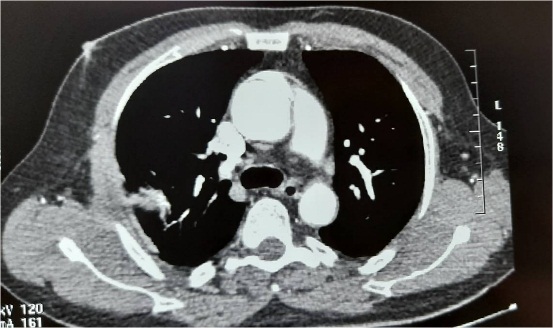
Figure 1 : CT scan showing the dissection of the ascending aorta.
Emergent trans-thoracic echocardiography confirmed the localized dissection of the ascending aorta without pericardial effusion.
The coronary dissection was treated by deploying 5 stents.
Then, the patient underwent emergent surgery with cardiopulmonary bypass between arterial femoral cannula, and atrio-caval femoral cannula.
After aortotomy, the intimal tear was sutured by a pledgetted suture without prosthetic replacement of the ascending aorta (figures 2 and 3).
The postoperative course was uneventful, and the patient was discharged 5 days after operation.

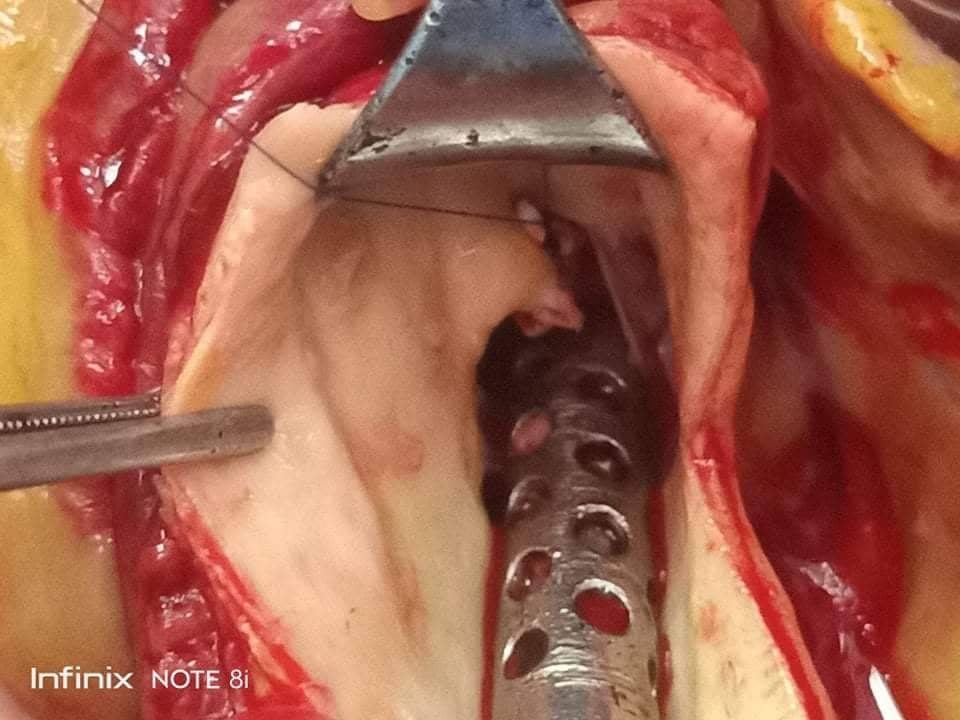
Figures 2 and 3 : Intra-operative views showing the intimal tear repeared by a pledgetted suture.
Discussion :
Iatrogenic aorto-coronary dissection is a rare but devastating complication with a significant impact on mortality of patients undergoing percutaneous coronary angioplasty [2].
It can be due to coronary stent dislodgement in calcified coronary arteries, a guiding catheter or guidewire, vigorous hand injection of the contrast medium, subintimal passage of guidewires, and inadvertent handling of the guiding catheter [3, 4].
Dissection at the ostium could propagate antegradely and result in total or subtotal occlusion of the coronary arteries without antegrade blood flow. It could extend as well retrogradely into the sinus of valsalva and cusp, compromising other coronary ostia, and propagate to the ascending aorta, aortic arch or even the descending aorta [5].
Many authors believe that if the aorto-coronary dissection is limited to the localized area, stenting on the intra-coronary entry point of the dissection is the most effective method of resolving this complication [1, 6, 7].
Dunning et al [8] proposed a classification for iatrogenic aortic dissection based on the extent of aortic involvement. Class I is defined as a focal dissection restricted to the coronary cusp. Class II involves the cusp and extends less than 40 mm into the ascending aorta, and class III extends from the coronary cusp up the ascending aorta greater than 40 mm, such as the case of our patient.
In class I and II lesions, sealing the entry port of the coronary dissection with a stent can prevent the progression of dissection [9].
When the lesion extends up the aorta > 40 mm from the coronary ostium, surgical treatment is usually required [1]. The objective of surgery is to repair the intimal tear with suture, without necessity of replacing the aortic segment dissected like in the spontaneous dissections.
Conclusion :
We describe a rare case of coronary artery and aortic dissection simultaneously occurred during percutaneous coronary intervention for a calcified lesion in the proximal right coronary artery. The situation was rectified by urgery under cardio-pulmonary bypass.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org