Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Rajshree Dayananad Katke
Department of Obstetrics and Gynaecology, Grant Govt Medical College and Sir JJ Group of hospitals, Mumbai, Maharashtra, India.
*Corresponding author: Rajshree Dayananad Katke, Department of Obstetrics and Gynaecology, Grant Govt Medical College and Sir JJ Group of hospitals, Mumbai, Maharashtra, India.
Received: January 18, 2021
Accepted: January 29, 2021
Published: February 16, 2021
Citation: Rajshree Dayananad Katke, (2021) A Rare Case Report of A Giant 30 Kg Spindle Cell Tumor Of The Uterus With Leiomyomatous Variant: World's Extremely Largest And Rare Tumor With Review of Literature.. Clinical Case Reports and Clinical Study, 2(2); DOI: 10.61148/2766-8614/JCCRCS/017
Copyright: ©2021 Rajshree Dayananad Katke, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Ovarian lesions composed of spindle cells comprise a heterogeneous group; benign as well as neoplastic. Abdominal-pelvic masses containing spindle cell and fibroblastic proliferation are very rare. Since limited studies have reported on the pathologic characteristics inherent in this disease, appropriate clinical management is undetermined.it also mark the importance of immunohistochemistry analysis of the specimen for confirmatory diagnosis.
Introduction
Low-grade pelvic masses with spindle cells and fibroblastic proliferation are very rare, poorly recognized, and not well described in the literature [1]. This histologic subtype has been associated with anaplastic thyroid carcinoma, medullary thyroid carcinoma, but also can reportedly manifest itself as a low-grade fibrosarcoma, malignant fibrous histiocytoma, myxofibrosarcoma, and fibrosing-type fibrosarcoma [2,3].
We describe herein the reported case involving the diagnosis and clinical management of a patient with low-grade abdominal pelvic masses exhibiting spindle cell and fibroblastic proliferation.
Case Presentataion
A 45 yr female , unmarried , nulligravida , known case of hypertension controlled on anti-hypertensives came to my outpatient department , with complaint of huge lump in abdomen and difficulty in breathing since 3 months.
Patient was a/a 3 months back when she developed swelling over pelvic region, insidious in onset, initially small in size ,gradually progressive to present size, painless .patient developed swelling over b/l lower limbs since 2-3 days, insidious in onset , gradually progressive. Patient is a k/c/o hypertension on tab clinidipine 10mg + chlorthalidone 12.5mg+ tab olmesartan 40mg patient also complained of dyspepsia and bloating sensation.
her sleep/bowel/bladder/appetite habits were unaltered her menstrual cycles were normal with her last menstrual period being 23.1.19.
Pt was admitted ON 24/1/19 in ward 32 I/V/O LUMP IN ABDOMEN SINCE 3 MONTHS.
on general examination , her vitals were stable. Pedal edema was present .No pallor / icterus / lymphadenopathy.
On per abdomen examination , the skin was distended hugely over abdomen with thinning and shining and over stretching of the skin. mass extending from lower pelvic region to xiphisternum and both the flanks were full and over filled. On per abdomen palpation , the huge mass was felt occupying the whole of the abdomen , arising from the lower pelvic area , extending to the flanks laterally and to the xiphisternum. There was no space left in the abdomen , the abdomen is full of mass. The mass is solid in consistency , margins were ill- defined , there is no shifting dullness. Because of the tense abdomen , mobility was restricted . On per abdomen percussion , dull note present all over the abdomen.
On per speculum examination- cervix was pulled up , os pin point on per vagina examination, it was consistent with the findings of per abdomen, the uterus was not felt separately.
On per rectal examination , rectal mucosa was free and same mass was felt.
All routine Investigations done and were normal. her Hb was 8.8 gm%. Xray ,ecg done- WNL
HCV,HBSag,HIV,VDRL NON REACTIVE.
25/01/19- ultrasonography of abdomen with doppler -impression : abdomen reveals grade 1 fatty liver , a large solid cystic lession is arising from the pelvis is extending upto epigastric region ,with thick internal septations. internal echoes are seen in the cystic lesion. The solid component shows internal vascularity. the uterus appears heterogenous in echotexture with multiple hypoechoic areas. b/l ovaries would not be visualised separately. the findings are suggestive of neoplastic etiology ,correlate with ca 125 levels. for further evaluation cect is advised.
28/1/19: Computed Tomography Abdomen : large heterogenously enhancing solid cystic septated lesion 23 x 34 x 38 cm extending from the pelvis upto epigastric region .the solid component shows heterogenous enhancement and measures approximately18.7 x 21.4 x 13 cms .b/l ovaries not seen separately findings s/o neoplastic etiology
tumor markers-
CA125- 238
CEA 4.85
B HCG <1.2
The case was thoroughly reviewed of history, physical
examination, and the final consensus for definite
management was radical surgery with a frozen report. Written valid informed consent was taken for the same.
Pre Anesthetic Check up was done. Patient declared fit for surgery.
On 4.2.19
EXPLORATORY LAPAOTOMY was done
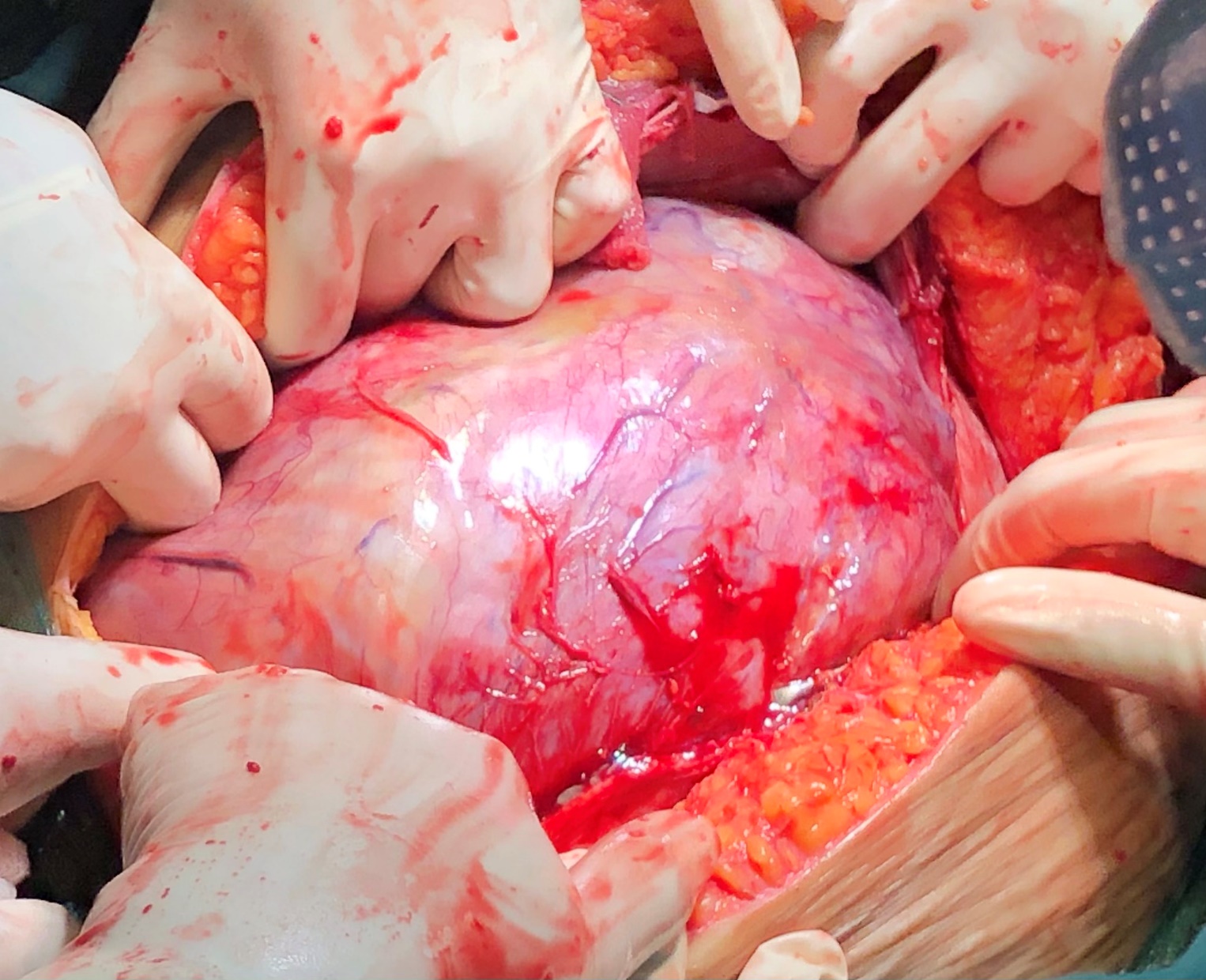
On per abdomen , huge mass involving all the quadrants in abdomen. upper border touching to xiphisternum and epigastrium. both flanks full extended to pelvis. (was like large mountain with approximately 40 x 50 x 40 cms). A supra umbilical incision was ten and after coming to the rectus sheath we have found that the rectus has thinned out, the rectus peritoneum and cyst wall was fused.

in situ findings
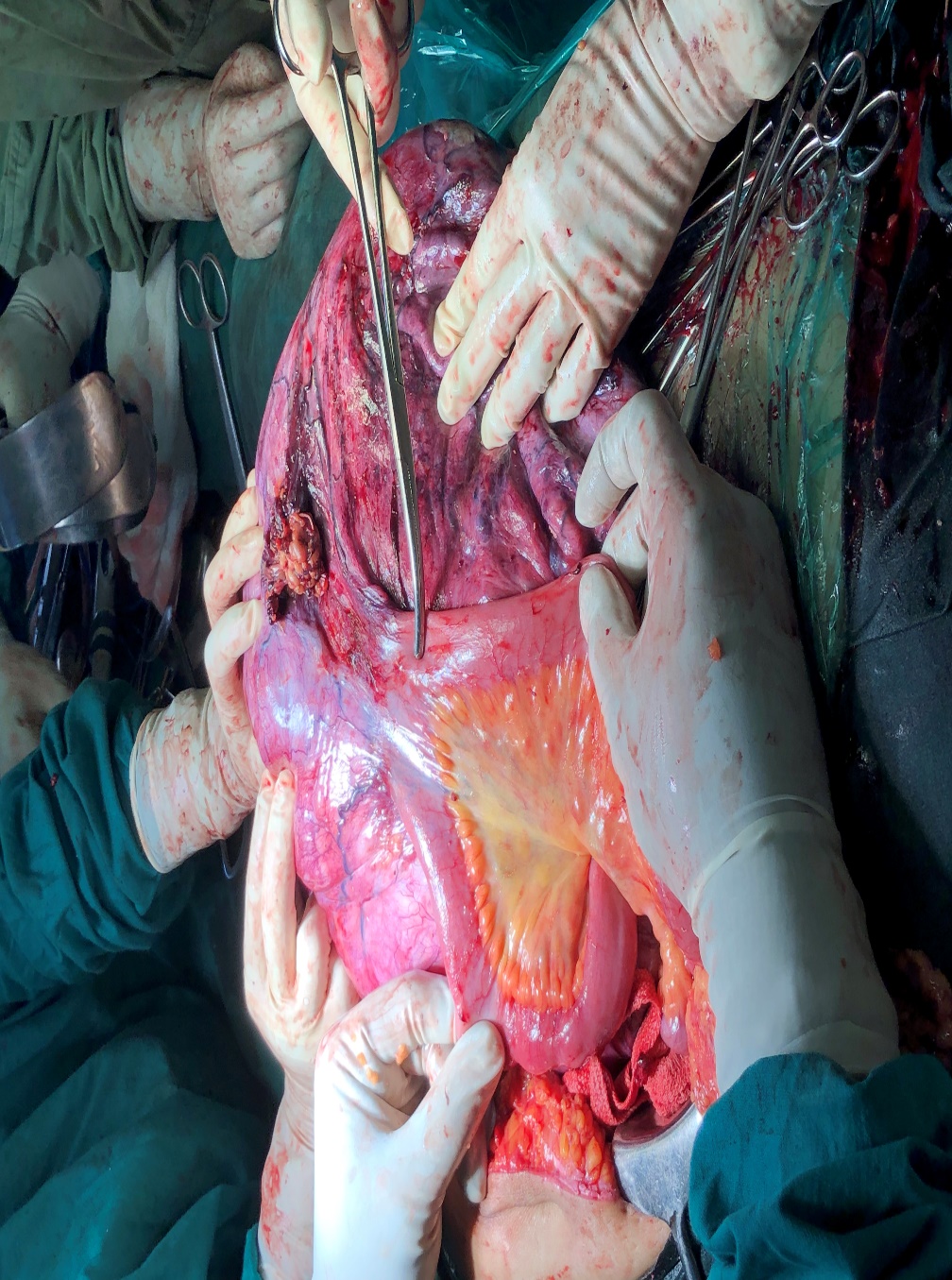
huge tumour extending to the diaphragm, liver, spleen, both paracolic gutter and lower part of uterus, dilated veins present ,mass was adherent to inner abdominal wall. no evidence of any ascitis. The mass had solid and cystic consistency and the mass was huge that it was not coming from the supra umbilical incision so the decisison of the part of cystic mass decompressed with the controlled suction, was taken and haemorrhagic cystic fluid was drained from the cyst , to reduce the volume of the mass which was n and huge fleshy mass has been delivered out. the mass, lower part was fused with uterus. The mass blood supply from bowel, omentum. weighing around 30 kg. to operate, the mass was separated from the uterus. the diverticulum, omental mesenteric adhesions were separated with ultrasonic and cautery, about 10-12 cm loop of bowel was flattened and densely adherant to mass and mesentric vessels were tied to save blood supply of that part of bowel but at the end resection anastomose was done because the bowel part was gangrenous and hence the total abdominal hysterectomy and bso done. frozen sent. s/o spindle cell neoplasm.
The final pathology revealed a huge spindle cell tumor with differential diagnosis being smooth muscle tumor (leiomyoma of deep soft tissue, mesenteric fibromatosis or extra intestinal stromal tumor)

The immunohistochemistry results showed spindle cells diffusely positive for SMA focally positive for Caldesmon and Desmin , weakly positive for CD10 and negative for inhibin and calretinin suggestive of a benign spindle cell tumor with leiomyomatous variant.
Post operative period was uneventful and patient was discharged after removal of stitches.
Discussion-
We report the rare status of a patient with low-grade abdominal pelvic tumors exhibiting spindle cell
Leiomyosarcoma is the most common malignant mesenchymal tumor of the uterine corpus. Tumor cells of leiomyosarcoma are spindle-shaped with characteristic cigar-shaped nuclei, or large pleomorphic resembling rhabdomyoblasts. Markers such as myo-D1 and myoglobin are more specific than muscle-specific actin, smooth muscle actin, and desmin, because smooth muscle markers have limited value in differential diagnosis. Undifferentiated endometrial sarcomas, highly aggressive neoplasms, do not histologically resemble entometrial stroma and may consist of spindle or markedly atypical tumor cells. Although CD10 expression has been observed in both uterine RMS4 and undifferentiated endometrial sarcoma, immunophenotypic evidence of skeletal muscle differentiation has only been seen with RMS. Mixed epithelial and mesenchymal tumors including adenosarcoma and carcinosarcoma consist of a mixture of benign or malignant epithelial and sarcomatous components. Epithelial components are usually glandular or rarely non-glandular and can be constitute a small portion of the tumor, especially in carcinosarcoma. Sarcomatous elements may be either homologous or heterologous with heterologous components frequently exhibiting rhabdomyoblastic differentiation 1
intravenous leiomyomatosis was first described by Birch-Hirschfeld in 1896 and defined by Norris and Parmlyin in 1975. 2
The neoplasm may result from the invasion of myometrial sinuses by either leiomyomatosis cells or proliferating smooth muscle cells, arising directly from the venous wall of the uterine or pelvic veins. 3
Most of the patients present in the 5th and 6th decades of life. Female gonadal steroids play a major role in the pathogenesis as the condition is associated with high estrogen levels. 4
Koh et al. studied two cases of low-grade fibromyxoid sarcoma with MRI, reporting that these sarcomas are rare and often quiescent, yet still have the capacity to metastasize 4
Hansen et al. described a group of 85 low-grade fibrosarcomas, which contained fibromyxoid, spindle cell or sclerosing epithelioid characteristics 5. Since this was a pathology study, there was no discussion regarding clinical management for the seven cases that developed recurrent disease.
The broad ligament is the most common extrauterine site for the occurrence of leiomyoma but with a very low incidence rate. Because of its overall low incidence rate, it poses both clinical and radiological difficulty in differentiating with an ovarian tumor. Hence, such tumors are extremely rare and good clinical hand and use of Doppler and MRI will help in planning surgical management 6
Atypical and bizarre leiomyoma synonymous with symplastic leiomyoma are rare smooth muscle tumors that contain cells with moderate to severe cytological atypia, but cell necrosis is absent and mitotic index is fewer than 10/10 hpf. Histomorphological features of atypical (symplastic) leiomyoma closely mimic leiomyosarcoma, and immunohistochemical markers are certainly of help to exclude malignancy in case of dilemma.7
Spindle cell sarcoma is a rare tumor that arises most commonly from the peripheral and deep soft tissues. It can present as a large abdominal mass.8
Mucinous cystadenomas may reach huge size as a matter of fact; many of the largest human tumours belong to this group. Grossly these tumours appear as rounded, ovoid or irregularly lobulated growths with a smooth outer surface of whitish or bluish white hue. Frozen section is very important to know the malignant variation of this tumour and that helps in the management of the patient. As in the huge tumours, the anatomical planes get distorted, so the surgical expertise is required to prevent the complications.9
The woman in our case study initially presented with a huge abdominal pelvic mass .and underwent surgical resection of her lesions. The final pathology revealed a benign spindle cell tumor with differential diagnosis being smooth muscle tumor (leiomyoma of deep soft tissue, mesenteric fibromatosis or extra intestinal stromal tumor) . The immunohistochemistry results showed spindle cells diffusely positive for SMA focally positive for Caldesmon and Desmin , weakly positive for CD10 and negative for inhibin and calretinin suggestive of a leiomyomatous tumour.
The uniqueness of this case is a huge 30 kg abdominal mass with a benign histopathological diagnosis and a very few such cases of this sort being reported till date.
Conclusion:
This is a rare case of benign abdominal mass reported till date a 45 year old unmarried women . more and more such cases are to be reported in literature so that a better clinical diagnosis and management is done. The importance of immunohistochemistry studies cannot be concealed. such cases require a very good surgical expertise and availabiltity of well equipped set up and good electro surgical unit s and instruments. The availability of frozen section highlights about the nature of tumor , so it is important to do the frozen section. In our case scenario , it was such a huge mass that the patient was unable to breathe and with good surgical expertise , we operated her nicely. Surgical assistance was taken for resection and anastomosis.
Conflict of interest ; none
Funding : none














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org