Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Mohammed Abdul Qader Alamalmi 1*, Med Bernard Rudger Blada 2
1Assistant prof. of dermatology and venereology in Al-Kuwait University Hospital Sana’a University Medical School, Republic of Yemen,
2chief of dermatology and venereology department in Augsburg Zentral Klinikum Germany.
*Corresponding author: Mohammed Abdul Qader Alamalmi, Assistant prof. of dermatology and venereology in Al-Kuwait University Hospital Sana’a University Medical School, Republic of Yemen.
Received: September 05, 2021
Accepted: September 19, 2021
Published: September 21, 2021
Citation: Mohammed Abdul Qader Alamalmi, Med Bernard Rudger Blada “Balanitis: due to bad hygiene inYemeni Men’s.” Clinical Case Reports and Clinical Study, 5(4); DOI: 10.61148/2766-8614/JCCRCS/091
Copyright: © 2021 Mohammed Abdul Qader Alamalmi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background: Balanitis is a common acute or chronic inflammation of the glans penis among dermato-venereological and genito-urinary medicine clinic attendees.
Objective:
General Objectives:
To study the pattern of balanitis in Sana'a city Al-Kuwait University Hospital Republic of Yemen from November 1996 to December 1998. Specific objectives: 1-To find out the causative factors of balanitis in Yemeni males. 2-To compare the proportion of balanitis in Republic of Yemen with the other studies fulfilled in Latin America, North America, Europe, Japan, Singapore and India.
Patients and Methods:
151 Yemeni male patients 16-60 years old presented with itchy and non-itchy erythemato-papular, pastulo-vesicular, erosio-ulcerative, plaque and scaly skin lesions in the glans penis of months and years duration. Serological tests for syphilis and H1V, skin scraping for mites, yeast and fungi, germ test tube, sab. Agar media stool and urine analysis, Gram-ve, Gram+ve staining, blood agar media, tzanck smear, random and fasting blood sugar was fulfilled. Skin biopsy with subsequent histopathological examination was in all selected patients.
Results:
The clinical data, investigations and the hisiopathological findings showed that 151 male patients suffered from irritant balanitis 9 cases )contact dermatitis 5 cases, fixed drug eruptions 4 cases), infective balanitis 131 cases (scabeitic 50 cases, candidal 50 cases, GBBUS 16 cases, stapylococcus aureus 2 cases. HPV 2 cases, herpes simplex progenitalis 7 cases, molloscum contagiosnm 4 cases) and oilier chronic unresolving conditions of balanitis 11 cases (psoriasis 5 cases, lichen planus 3 cases, lichen nitidus 1 case, lichen sclerosus et atrophicus 1 case, squamous cell carcinoma 1 case.
Conclusion:
Balanitis is a common skin disoreder in Yemeni males. The most cases are caused by infection, with scabies female mites and Candida albicans and the married individuals are more affected than singles. This is due to the high poor sexual hygiene in the two partners. GBBHS, staphylococcus aureus is common and there are a wide variety of other rare infective causes. In addition, irritant and other chronic unresolving conditions of balanitis are contributing factors.
Introduction:
Balanitis or balanoposthitis is a common skin disorder of the glans penis in the uncircumcised and circumcised males in the genito-urinary medicine clinic attendees. Irritant, infective, traumatic and chronic unresolving conditions cause many cases of balanitis [54]. Of the 51 patients diagnosed as having mild balanoposthitis, the cause was ascertained in 34 cases (infection, mechanical, trauma, contact irritation, contact allergy), whereas no specific aetiological factor was detected to explain the symptoms in the remaining 17 cases [130]. Neglected hygiene and tight foreskin cause balanitis and seborrhoeic dermatitis commonly seen on the skin folds. Thrush (candida), contacts allergy, balanitis xyrotica obliterans (lichen sclerosus et atrophicus), balanitis circinata and diabetes. Generalized skin conditions cause balanitis including lichen planus, psoriasis, erythema multifome, erythema fixum (particularly cause by tetracycline antibiotics) and erythroplasia of Queyrat (a rare precancerous skin condition). [74] Diabetes is the most common underlying condition associated with balanitis. The other causes include personal hygiene, chemical irritants (soap, petroleum jelly), edematous conditions (right side congestive heart failure, cirrhosis and nephrosis), and drug allergies (tetracycline, sulfonamide) arid morbid obesity. Penile cancer: several organisms and viruses cause balanitis including; candidal species (most commonly associated with diabetes), anaerobic, infection human papilloma viruses gardenerella vaginalis, treponema pallidum (syphilis), trichomoiial species, group B stieptococcoi and borrelia vincntii. The differential conditions of balanitis are phymosis, paraphymosis and psoriasis. The oilier conditions considered balanitis are lekoplakia, lichen planus, and Reiter's syndrome. [6]. The most common causes of balanitis are candidiasis, parakeratosis circinata, erosive circinata, gangrenous phagedaenica, pseudoepillieliomatons et keratosis, ulceration, balanitis xyrotica obliterans, candidomycosis and soorbalanitis. The other conditions cause balanopostliitis are acute (infection, contact allergies), candidomycosis, clironic (circumscripta benign plasmacellularis and diabetes. [5]
For the above-mentioned studies it is obvious that there were irritant, infective, traumatic causes of balanitis. In those studies, some authors regarding psoriasis, lichen planus, lichen nitidus. Lichen sclerosus et atrophicus and sqaumous cell carcinoma causes of balanitis and the others considered these conditions as deferential. Candidal balanitis was noted common in uncircumcised males with or without diabetes mellitus in Europe and America. This study which started in November 1996 and was completed in December 1998 may clarify the pattern, causative factors and proportion of balanitis in Yemeni circumcised men.
Definition of balanitis:
Balanitis is an acute or chronic inflammation of the glans penis "Posthitis" refers to an inflammation of the mucous surface of the prepuce. The term balanoposthitis thus refers to an inflammation of the penile skin. [10]
Pathogenesis of balanitis:
There are several factors that predispose to balanitis, smegma, urine, alkalis, and external contacts; friction and trauma; a long foreskin combined with poor hygiene; and exposure to venereal and vaginal pathogens. Bacteria, yeasts, and fusospiral organisms are abundant in the -perpetual sac and although normally saprophytic, may, under conditions of lowered local or general resistance, become pathogens. Chlamydia and mycoplasmas are being increasingly identified as the pathogenic organisms in balanoposthitis. [131].
Histopathology of balanitis:
There are histologic features characteristic of balanitis. General features of an inflammatory response predominate with a dermal infiltrate. Spongiosis may be present. [130]
Clinical picture of balanitis:
Balanitis manifested with pain, redness and swelling of the head of the penis. [131].
Historical Review of balanitis
Infective balanitis
Fungal infection and balanitis
Candidal balanitis:
Candidal balanitis considered to be the most common cause of balanitis and is due to infection with candidal species, usually Candida albicans. It is generally sexually acquired although carriage of yeasts on the penis common, being 14-18% with no significant differences between carriage ratein circumcised or uncircumcised men. Symptomatic infection is more common in the uncircumcised male- Significantly more of the female partners of men carrying yeasts were found to have candidal infection- [39,115] Diagnosis may be on the clinical appearances alone, microscopy and/or culture. The sensitivity of microscopy varies with-method of sampling, and an "adhesive tape" method has proven to be more accurate than swabbing. Infection may occur without sexual contact, usually in the presence of diabetes of which it may be the presenting symptom, or after the use of oral antibiotics. [45,135]
Symptoms are of burning and itching of the penis with generalized erythema of the glans and/or prepuce which may have a dry glazed appearance, with eroded white papules and white discharge. [105]
In diabetic papules patients the presentation may be more severe with oedema and fissuring of the foreskin, white may become non-retractile. [134] Candidal balano-posthitis is a well recognized condition, first described. [55,59] performed the classification of balanitis candidomycetica on the basis of thirty two cases and the forms included Small pustule, diffuse erosive form, erythematous form with maceration of epidermis, erythematous form with maceration scaling and membrane, erythematous membrane, erythematous form with desquamation, small papule form, sour form, balanitis purulent candidomycetica, eczematiod form, chronic infiltrate form with desquamation, ulcerative form and candidogranuloma of penis. Candida is a common cause of balano-posthitis- Diagnosis by microscopy has a low sensitivity and varies with the method used for collecting material. Although up to one third of genitourinary medicine clinics may rely solely on clinical appearance for diagnosis most continue to use microscopy and culture. [45]
Treatment:
Genital candidiasis in men should be treated with saline washes or local applications of an antifungal cream. Nystatin should be applied morning and evening for at least two weeks. Clolrimazole, miconazole or econazole creams should be applied for at least one week. Female partners should also be investigated. Men who fail to respond to treatment should be referred to a specialist for investigation for other infectious or non-infectious causes of their condition. Long term antifungal treatment may be appropriate for those with recurrent penile candidiasis associated with catheters or drainage devices. Treatment can be topical (for example clotrimazole), or oral such as with fluconazole but partners should be screened as they have a high rate of infection. [39] The patient's sexual partner must be treated as well as the patient. If underlying factors are causing the infection, these may need to be addressed. This could mean better hygiene, or in persistent cases, an evaluation for diabetes. Mild cases of candidal balanitis with respond to cool bathing with Burow's solution and antifungal cream. Most topical antifungal compounds are acceptable; oral nystatin or ketoconazole for a week or two may be considered, to decrease gut and perennial colonization. [33] The small preliminary study suggests that single dose oral fluconazole is an effective, well-tolerated and convenient treatment for penile candidiasis. Larger studies comparing fluconazole with existing topical therapy for penile candidiasis should now consider. [90, 91]
Bacterial infection and balanitis:
Streptococci:
Group B streptococci can be carried asymptomatically in the adult genital tract, but strongly associated with balanitis. Rate of carriage varies between heterosexuals and homosexuals (16.6%) in heterosexuals and 39.3% in homosexuals) although no balanitis occurred in the latter group. Sexual transmission is unclear as there was no expected age differential in one study and in another meatal carriage was proportional to promiscuity. [8, 17,132] The clinical appearance is of nonspecific erythema with or without exudate, but more rarely may extend to penile cellulitis if abrasions are present. [97] Group A haemolytic streptococci have also been reported as causing balanitis. Most reports are of uncircumcised children who presented with erythematous, moist balanitis. [42, 73. 93] Where the mode of transmission appears to be autoinoculation from other sites pyoderma of the penis following fellatio has been reported, and in this case group A haemolytic streptococci were isolated from the coronal sulcus. Penicillin or cephalosporins are effective in treatment. [50]
The foreskin was trimmed to allow drainage of the abscess and excision of the sinus. Regular dressings were applied until healing had occurred, and circumcision was performed 6 months later. He has had no recurrence of his pilonidal abscess after 2 years. The men attending in genitourinary medicine clinic had an appreciably higher prevalence of subpreputial infection with group B. streptococci (GBS) than with Staphylococcus aureus or coliform bacilli. Carriage of GBS was similar in older and younger age groups and was higher in homosexual than heterosexuals and in those with balanitis than those without. Thus, while GBS mat because balanitis in heterosexuals, sexual transmission is unimportant; in contrast sexual transmission of GBS may be more common among homosexuals but balanitis is rare. [8] Group A B-hemolytic Streptococcus can cause balanitis in prepubertal males, and its incidence is probably greater than previously reported in the pediatric literature. Group B B-hemolytic streptoccci (GBBHS) are known to be able to colonize the male urethra, but this organism has not previously been isolated from cases of balanitis. [16] Two cases reported in which Lancefield group beta-haemolytic streptococci were isolated from culture from the perianal skin. The physical examination showed perianal irritation and excoriation in both cases and seropurulent anal and balanopreputial discharge in the first only. To the best of their knowledge this is the first case in which the streptococcal perianal disease is associated to a balanoposthitis and at the same time increments the clinical spectrum of the illness. [129] Three boys with balanoposthitis, with and without discharge, were diagnosed and treated at a private pediatric office in a recent 16-month period. The experiences of these and other patients enabled the authors to draw several conclusions concerning effective diagnosis of this condition. Attention to these clues can usually identify boys in whom the diagnosis of sexually transmitted disease is highly unlikely and avoid the necessity of unneeded laboratory tests. However, it is advisable to perform a test for S. pyogenes, because streptococcal balanoposthitis may be indistinguishable from the more common condition caused by inadequate local hygiene. Streptococcal balanoposthitis need not produce a discharge. Other than cases of streptococcal etiology or sexually transmitted diseases, most boys with this condition can be managed by attention to local hygiene and, in some cases, use of a mild hydrocortisone cream. [121] A 5-year-old boy who was admitted with a history of 12 months of anal and preputial discharge not related to defecation or urination and associated with intense perianal and preputial erythema. [73] One case of balanitis caused by Group A betahemolytic Streptococcus reported. They were not able to find in the literature a report of balanitis caused by Group A betahemolytic Streptococcus in a prepubertal boy. Prompt identification of the organism is essential for appropriate early treatment. [42] The first description of streptococcal balanitis in a healthy adult and should alert other physicians to-the importance of a more active search for GAB HS in glans discharges. As more cases of streptococcal balanitis are identified, they will be better able to define the pathogenic role of this GABHS. [106]
Staphyloccocus aeureus:
This has infrequently been reported as causing a balanitis, although carriage is not strongly associated with symptoms. [1. 8, 50, 107]
Two cases of staphylococcus aureus infections presenting as inflammation of the median raphe of the penis and suppurative inguinal lymphadenitis are described. Both conditions resolved following treatment with flucloxacillin. [107]
Treatment:
Bathing with cool Burow's solution and a topical antibiotic will decrease the inflammation. [33]
Viral infection and balanitis
Herpes simplex viruses:
In rare cases primary herpes can cause a necrotizing balanitis, with necrotic areas on the glans accompanied by vesicles elsewhere and associated with headache and malaise. This has been reported with herpes simplex virus types 1 and 2. Almost 90% of genital infections in men are caused by herpes simplex virus type 2 (HSV-2) strains- in one-third of these patients the HSV-2 infection occurs in the absence of antibody to either HSV-1 or HSV-2. They describe all unusually server primary HSV 2 infection in a 37-year-old man. Healthy, 26-years old heterosexual man had penile ulceration with fever, rigors, and difficulty voiding urethral trumentation and treatments with antibiotics were associated with progression of the disease. HSV-1 was isolated from the penile ulceration and pustular lesions in the groin and antecubital fossae. Recovery was complicated by a urethral stricture requiring surgical treatment. HSV- 1 must be considered in the differential diagnosis severe penile ulcerations; isolation of herpes virus from such lesions may need further diagnostic and therapeutic measures that are unnecessary in some cases, counterproductive. [109,112]
Many individuals with genital HSV infection reported that they are able to predict at least a proportion of attacks through warning prodrormal sensations. However, the frequency and reliability of such sensations is not known. (Brookes and Green; 1992)
There is a positive relationship between absence of circumcision and genital HSV infection, but that a prospective study should be undertaken to confirm these results. [127] The patients come for treatment for their recurrent involvement of genitals with no apparent reasons according to them; main complaints were of vesicles formation preceded by itching for 2/3 days. As a result of itching vesicles ruptured leaving behind an erosive, erythematous and a little oedematous glans penis with subpreputial serous discharge. Sometimes, someone complained of pain. Only two cases out of twenty-two herpetic balanoposthitis had inguinal lymphadenopathy, involving either side by each. It was possible to isolate herpes virus from only three cases out of six intact vesicular herpetic balanoposthitis.Histological findings of herpetic genitalis in epidermal vesicles formation with profound degeneration of epidermal cells to resulting to acantholysis. Multinucleated balloon cells were found in the base of the vesicle together with the reticular degeneration in the upper portion of the vesicles. Upper dermis showed inflammatory infiltrate. The picture was typical of viral vesicles. In cases with ruptured vesicles-three was lotus of epidermis with dense infiltration mainly with lymphocytes and a few neutrophils. [27]
Treatment:
Acyclovir is very effective in suppressing recurrent genital herpes and is clearly superior to isoprinosine, which is not clinically useful in the dosage. [89]
Human papilloma viruses. Papilloma virus may be associated with a patchy or chronic balanitis, which becomes acetowhite after the application of 5% acetic acid. [4, 11] Acetowhite change has also been reported in non-HPV associated balanitis and has resolved on treatment. [72] HPV was identified in two studies—in the first in 56% of patient samples (of which 54% were oncogenic types) but only 26% of controls, and the oilier revealed HPV6 in 4 out of 5 cases. [11,136] Nearly one-third or 30.5% of these randomly selected patients in Swedish STDs clinic were infected by HPV. The diagnosis was made by clinical inspection and/or by HPV DNA analysis with polymerase chain reaction (PCR). [125] Fifty patients presenting with either primary or recurrent patchy balanoposthitis, which became aceto-white after the application of 5% acetic acid underwent biopsy. Microbiological screening, including Grocott staining of the biopsy material for fungal hyphae was performed. Forty-nine biopsies showed marked leuccytosis suggestive of human papilloma virus (HPV) infection, and of these, only three showed fungal hyphae. This study suggests that HPV may be associated with some cases of patchy balanoposthitis. [4] HPV DNA was distributed widely in the anogenital area, in warts, acetowhite areas and clinically normal skin. The SG technique was well tolerated by patients and produced results consistent with other findings. Sampling from a single site of the genitalia on one, occasion may significantly underestimate the infection rate with IIPV. Multifocal infection of the anogenital areas with HPV should be taken into consideration when interpreting epidemiological studies and management strategies. They found that the HPV is present in the urogenital tracts of men with gonorrhoea, penile warts and with genital dermatosis. In men with urethral gonorrhoea, detection of HPV in urethral specimens is not related to the number of sexual partners, condom usage, racial origin or past history of genital warts. HPV DNA in the urethral swab and urine specimens may represent different aspects of the epidemiology of HPV in the male genital tract. The preponderance o HPV types 16 and 18 in all three groups of men may be relevant to the concept of the "high risk male". [80] The "high-risk" HPV types are prevalent in papular and especially macular penile condyloma-like lesions. The histological finding of koilocytosis concomitant with dysplasia strongly indicates infection with a "high-risk" HPV type. Although the risk of penile cancer is low, it is from an epidemiological point of view important to diagnose these lesions. Until simple tests for HPV typing are available, biopsy for light microscopy (histology) should be obtained liberally from papular and macular condyloma- like lesions. In atypical cases of balanoposthitis HPV etiology should also be considered. [96] Genital papilloma viruses do not have a strong association with balanitis xerotica oblitrans (BXO). Symptoms included redness, itching, burning, tenderness, dyspareunia, fissuring and in two cases penile oedema and inguinal adenopathy. All patients fulfilled penoscopical and histopathological criteria for HPV infection. Demonstrate some tentative evidence that HPV might be associated with long-lasting balanoposthitis, although their data still are circumstantial for a causative association. [96,136]. Patients must first be told the nature of their problem and that it is a sexually transmitted disease- It is strongly advised that a patient's sexual partners, particularly woman, be screened for disease in view of the oncogenic potential of this virus. [32]
Partners should be treated concurrently, as this infection can easily be passed back and forth. Men should use condoms while being treated to avoid spreading the virus and being reinfected. The patient must also be warned prior to treatment that these infections are often recalcitrant and that it may take many visits to control the infection. Penile genital waits may be almost invisible, particularly if they are of the flat variety. A motivated patient is a great asset and many such patients will gladly mark with ink suspicions areas before their appointments. An aid is 3 to 5 per cent acetic acid solution, which will turn many previously invisible, slightly hyperkeratotic lesions white if the area is soaked with saturated gauze for 5 minutes prior to examination. [31] In their experience, however, the lesions do not become dramatically more visible. This solution may cause scrotal irritation, which can be alleviated with brisk irrigation. Magnification lenses (3 to 5x) are also useful to see smaller lesions. [35] If a patient has perirectal warts, a sigmoidoscopy with destruction of internal warts should be performed before potentially painful external therapy is undertaken. Internal warts, which are present in 50 to 70 per cent of men who proactive anal intercourse and have perirectal warts, will cause rapid re- infection and so should be eliminated first. [26] Persistent recurrent meatal warts may be indicative of urethra condyloma, which ranges in incidence from 5 to 23 per cent in those cases. Principle also applies to intravaginal or cervical warts. [41] Pobophyllin, 10 to 25 per cent, usually in benzoin, is still the first choice for treatment despite its oncogenicity and potential other toxicity. It is particularly effective for young moist warts and less so for mature hyperkeratotic ones, although pretreatment of the latter with monochloroacetic acid will render them much more susceptible to the drug. [56]. Podophyllin is painted on (lie wart and allowed to dry before releasing (lie skin of the penis. Some authors advocate the application of baby powder or a like substance to prevent spread from the site of application. Sensitivity to the preparation varies among individuals and with the particular batch being used, as potency decreases with time. It is safest to wash off the first application after 4 hours, and, if it was well tolerated, to lengthen the contact time thereafter. [69] At least four to six applications are usually required for a cure. Biopsies of warts that have been treated with podophyllin can be misleading, as histopathologic changes consistent carcinoma in situ can be present. [60] It is dangerous to apply podophyllin in a widespread manner to mucous membrane surfaces as absorption and systemic toxicity can occur. Usually in women Physicians should also take care not to spill the podophyllin on their fingers, as it will adhere most tenaciously and can cause a severe Conjunctivitis if later rubbed in the eyes. [40] Destruction of the warts by heat or cold is a useful method of treatment out is more painful than podophyllin. Excision with figuration of the base is adequate therapy, and tissue for pathologic confirmation can obtain. If there are many lesions, however this approach can be some impractical. [25] Liquid nitrogen can be applied by a variety of devices, but none surpasses a cotton swab and a Styrofoam cup. The wart is frozen solidly twice, including a small rim of apparently normal tissue. The warts will blister, new skill will grow from underneath and the warts will fall off. Potential hazards include hypopigmentation, particularly in black patients a small risk of scaring and, rarely infection. [66] Electrodesiccation can also be used after individual warts are anesthetized. Warts bubble in a Characteristic manner and the margin of warty tissue becomes evident upon treatment. Hypopigmentation and scarring are a risk if the thermal injury extends into the dermis [63] Recently, carbon dioxide (CO2) laser therapy has been successful for recalcitrant venereal warts. The later has several advantages over electrodesiccation, including exact control of tissue destruction, a bloodless filed, a sterile wound after surgery, and less postoperative pain, presumably because of sealing of nerve endings. The laser call also the laser can also be used to abrade (lie area around the wart lightly. [24, 66, 114, 117, 118] This step can increase cure rates particularly for lesions in the perirectal area, as wart virus can lie latent in the superficial epidermis well away from the obvious warty growth. [60] Previous reports of results with the laser, with cure rates of 90 to 100 per cent, may have been optimistic, however, as a recent study of the C02 laser, acetic acid soaks, and an operating microscope indicated a recurrence rate (albeit often microscopic) of 66 per cent. [25] The disadvantages of the laser include possible hypopigmentation and scarring the need for anesthesia, high initial expense, possible ignition of drapes and clothes, and the need for protective goggles. Also, a plume of smoke, in which intact papilloina virus can he identified, is created with the CO2 laser necessitating aggressive smoke evacuation. The wearing of masks while performing laser surgery on warts is advisable, but masks will not filter out the tiny particles created by the laser. The risk of inhaling this plume of smoke is strictly theoretical but unpleasant to contemplate. [3] More recently, interferon therapy has been successful in treating condylomata. Intralesional interferon alpha-2b was used by one group with fair results, but it requires multiple injections and is associated with systemic side effects including fever, chills, myalgias, headaches, fatigue, and transient leukopenia. [56] Human lymplioblastoid interferon has been used systemically (intramuscular injections) in women with recalcitrant condylomata., with about half of the lesions clearing completely after 34 injections 3 Side effects were similar to those noted above. To their knowledge, interferon has not been tried in giant condyloma, but tilts might be one lesion where it would be very useful, as conventional therapy is currently than ideal. [67]
Molluscum Contagiosum:
Molluscum contagiosum is caused by a poxvirus that can be spread by casual contact in children but is usually spread by sexual contact in adults. The lesion is a characteristic 3- to 6mm dome-shaped, pearly papule with a central umblication. These lesions may be found on the penis or the perigenital area. A white curd-like core can be expressed from many of the lesions that contain many highly infectious viral particles. Lightly freezing suspected lesions will aid diagnosis, as the edges of the lesion are accentuated, and the central cell revealed. [20]
Treatment:
This infection resolves spontaneously after 3 to 4 months in many patients, but this wait is not usually acceptable to patients or parents. Moreover, autoinoculation can occur, as can scarring, if excoriated lesions become secondarily infected. Molluscum can easily be scraped off with a sharp curette without anesthetic or lightly frozen with liquid nitrogen and will heal without scarring- It may take repeated sessions to clear the infection. [3] Parasitic infection and balanitis
Scabies:
Scabies is caused by thy mite sarcoptes scabiei var. hominis and has plagued mankind since antiquity. The mite is an obligate human parasite, and usually is transmitted by direct personal contact, although there are well-documented cases of transmission from heavily infected clothing or other fomites. [22] The diagnostic hurdle with scabies is maintaining high enough clinical suspicion to consider the diagnosis. Scabies infestations rarely involve the penis alone, and the patient will usually volunteer that he is itching mightily. [64] Skin lesions may be tiny papules, wheals, pustules, or vesicles. There are occasionally 2- to 15-mm straight, zigzag, or S-shaped burrows, usually excoriated, that are considered diagnostic by some authorities. Almost all lesions are excoriated, and patients commonly are secondarily infected. [33] The distribution of lesions is the key to correct diagnosis. Concentrations of activity are commonly been on the flexor wrists, in the finger webs and the sides of the fingers, on extensor elbows and anterior and posterior axillary folds, periumblicus, waist, periareolar area, lower buttocks, extensor knees,lateral feet, and in the groin. [22] The head and back are usually spared. Men usually have penile lesions, and (these are small erytheniatous, sometimes coppery or bronzed, slightly hyperkeratotic, papules that itch severely. [33] It is difficult to find and demonstrate a mite; most patients have only 3 to 50 mites at any given time. Therefore, most patients are treated on a suspicion basis. The best sites for scraping with a No. 15 blade are early papules and burrows. If a tiny blister is scrutinized very closely with a bright light, a dark female mite (speck) can sometimes be seen with the unaided eye. Mites, their eggs, and their characteristic feces (scybala) are easily seen with low-power microscopy if they are present. [86] The epidemics of scabies and human lice have been observed for centuries very little has been recorded about the epidemiology of the sexually transmitted forms of these diseases, which are seen commonly in sexually transmitted disease clinics. In the present study, attendees at a sexually transmitted disease (STD) clinic from 1988-1991 were examined for scabies and pediculosis pubis and a wide range of independent variables analyzed by multiple logistic regression to define independent correlates of infestation. In scabies appears to be determined by socioeconomic factors and pediculosis pubis predominantly by sexual activity factors. [76]
Treatment:
Adults can be safely treated with topical lindane (Kwell, Scabene) lotion rubbed in well from the chin down for two consecutive evenings before bed and washed off in the morning. Two ounces per adult usually suffices. All household members and close contacts must be treated, even if they show no symptoms of infection, as it may take several weeks for hosts to develop hypersensitivity to the mite and become symptomatic. Clothing and bedding should be washed with hot water the night of treatment. [12] Lindane should not be used on children under 1 year of age or on pregnant women because of possible neurotoxicily. Suitable alternatives are available. Crotamiton cream or lotion 10 per cent (Eurax), which may be irritating, is applied from the chin down. A second application is made, without washing off the first, at 24 hours, and the patient bathes after 48 hours. The oldest, safest, but least effective treatment is 5 to 10 per cent sulfur precipitates in petrolatum. [113]
This is a messy preparation that is best used in infants. It should be applied three nights in a row, bathing each evening before the next application. Special care must be taken with the periungual areas, as mites may be able to hide in the kerafotic debris that is often impacted there. [123] The patient must be warned that it may take two to three weeks for the itching to subside. Antihistamines and perhaps a topical steroid (triamcinolone 0.1 per cent cream) will help to tide them over. The penile scabies nodules may persist for months after effective treatment and may require an intralesional injection of dilute steroid solution (triamcinolone 3.3 mg per ml) for resolution [38]
Irritant and allergic balanitis:
Many balanitis is non-specific, and no etiological agent can be found. It has been suggested that these are often due to irritation, particularly if symptoms are persistent or recurrent. In one study of patients with persistent or recurrent problems72% were diagnosed is irritant balanitis, and this was associated with a history of atopy and more frequent genital washing with soap.[10] Other series have found higher rates of infective agents, although a large proportion of cases in one study remained undiagnosed .[1,130,58] It is likely that irritation plays some part in other balanitides. More severe reactions have been seen with topical agents, some of which may have been used for treatment. Dequalinium is known to cause a necrotic balanitis, while titanium (that was previously thought to be biologically inert) may rarely cause a granulomatous balanitis. [34, 52] Balanitis as an allergic reaction is very uncommon; rubber and its constituents are the most frequently described allergens, although allergy to spermicidal lubricants is also well described [81,128] There is a wide spectrum of clinical manifestations varying from balanitis to oedema of the whole penis extending to the groins. Treatment will depend on the seventy of the reaction, but patch testing and avoidance of the precipitant is required. [54] Many dermatological conditions may also have a predilection for the male genitalia. Psoriasis, lichen planus and seborrhoeic dermatitis are common and evidence of involvement its other sites should be sought. Dermatitis artefacta of the genitals has also been reported. Balanitis may occur with both Crohn 's disease and ulcerative colitis. Many balanitis proves difficult to diagnose and any condition which persists despite simple treatment warrants further investigation. Penile biopsy is easy to perform and is useful in these cases. In about 60 patients with unresponsive penile dermatoses underwent biopsy, of whom 26% had a non-specific dermatitis, 23% are virus infection, and 15% lichen sclerosus. The original clinical diagnosis was confirmed in 33% of cases and the biopsy was not diagnostic in only 3% of cases. [4, 82] Poor hygiene, retained soap, detergent, retained smegma or inadequate drying may cause an irritant dermatitis. Contact dermatitis affects the shaft rather than the glans, except when medicament or contraceptives are involved. [30] The application of quaternary ammonium as a local antiseptic causes necrotic balanitis. [53] The Smegma is fatty degenerated detritus of cells of the prepuce, with which repeated animal experiment results in development of cancer. By the child they must take into consideration two factors: 1. the retractibility of the prepuce without causing lesions and 2. The ability of independent retraction of the prepuce by boys before school age, formed four groups of kindergarten children and did compare them. The retroactivity of the prepuce developed from 71,0 % to 79,7 %, but the independent ability of these boys to retract their prepuces developed from 4,3% of the three years old boys to 72,9 % of the six years old boys. The education to wash their prepuces in this age is a principal task of the parents. These must be instructed by the medical officers not only to begin this practice at the proper time, they mean after the third year, but also to realize the right technique of hygiene while washing the prepuces to prevent lesions or inflammations. [111] The sexual hygiene of mental retarded boys exanimates. In comparison normal schoolboys is pointed out the necessity of sexual pedagogic education. [110]
Treatment:
The primary treatment of any contact dermatitis is to determine the allergen and avoid it. This may require exhaustive histories, patient logbooks, and patch testing. Rhus dermatitis usually requires 10 to 14 days of oral prednisone therapy. In less inflammatory reactions, application of topical steroids of low or medium potency will yield resolution in a few days a long- term solution for condom dermatitis may be more problematic. It may be possible to find condoms without thiuram accelerators, and there are animal products (sheep intestine) condoms are available. However, animal products have larger pores than rubber condoms and so may not prevent the spread of the human immunodeficiency virus. [33]
Fixed drug eruptions:
Fixed drug eruptions have a predilection for the glans penis and are commonly related to therapy with antibiotics especially tetracycline and sulfonamides. [46]
Oilier causes include salicyclates, phenacetin, phenolphthalein and some hypnotics, although there are case reports of other less common causative agents, for example.
Lesions are usually well demarcated erythematous areas which may be bullous and subsequently ulcerated. [15, 36, 37] This can occur on the first exposure to a drug and repeated exposure will precipitate new lesions at the initial site (this can confirm the diagnosis. [46] However, tetracycline induced eruptions may not recur on challenge with doxycycline. [37] Most lesions will fade spontaneously without treatment but may leave an area of residual hyperpigmentation. Occasionally treatment with topical, or rarely, systemic steroids may be required. [15]
Two cases reported of fixed drug eruption, balanitis thought to be due to co-trimoxazole (Scptrin) a mixture oftrimethoprim and sulphamethoxazole). [126]
The fixed type of eruption brought on by tetracycline frequently involves the glans penis and gives rise to a balanitis. He should like to report two cases of tctracycline-induced balanitis that did not recur with challenges to doxycycline and minocycline. [5]
Treatment:
Treatment is largely symptomatic. Pain medication may be required. Occasionally, urinary obstruction has been reported from edema. Avoidance of the offending drug is critical- Topical steroids may hasten the clearance of the inflammation. [33]
Psoriasis:
Psoriasis commonly occurs on the penis, and occasionally the penis is the only site affected. The preputial glans is the most common site involved. Red plaques with well-demarcated borders and a dull, velvety, granular surface are seen. The silvery scale commonly associated with psoriasis is usually not seen on the glans, particularly in the uncircumcised. Psoriasis in the shaft will have silver or amber scale. [88]
The most important diagnostic clue for psoriasis is a history or presence of lesions elsewhere psoriasis may be found on the scalp (dandruff), behind the ears, on the extensor elbows and knees, in the umbilicus, and in the gluteal cleft. There may also be numerous tiny pits in the fingernails. [33] Psoriatic lesions may be small scaly papules or large red plaques, almost always with a silvery scale. The differential diagnosis for penile psoriasis includes balanitis circinata (Reiter's syndrome), plasma-cell balanitis, erythroplasia of Queyrat and Bowen's disease, bowenoid papulosis, lichen planus, and fixed drug eruption. [88] Skin biopsy, although usually not necessary, will show parakeratosis, acanthosis, and capillary dilatation in the dermal papillae. [33] The genital psoriasis, especially of the glans penis, are frequent, difficult to treat, and disturbing to patients. The characteristic genital lesion is a well- demarcated pink plaque of the glans penis. More extensive lesions are sometimes difficult to distinguish from the balanitis of Reiter's disease. Psoriasis is a treatable and often overlooked cause of vulvar discomfort. Other mucosal sites are rarely affected. [124]
Treatment:
Psoriasis is usually a life-long affliction with a waxing and waning course. The penile lesions may be asymptomatic, and reassurance that these are not some dreaded venereal infection may suffice. If this is not sufficient, addition of a mild tar compound such as 5 to 10 per cent tar in Nivea lotion will help. It is convenient for some patients to mix a small amount of the tar preparation into the container of hydrocortisone so only one medication needs to be applied and to dilute the tar, so it is not so irritating. Balanitis circinata may be treated as in psoriasis mentioned above, although tar preparations may be irritating. [33]
Lichen Planus:
The hallmark of lichen planus is violaceous to purple polygonal flat-topped papules that itch. The cause is unknown. This is usually a generalized eruption, with involvement of the penis in 25 per cent of cases in males. Often, there are lacy reticulate lines on the buccal mucosa that aid in diagnosis. Penile lesions, in the absence of papules elsewhere, are rare. There are usually many, tiny, shiny, polygonal papules on the glans that can be difficult to tell from lichen nitidus. [88]
The papulosquamous lesions of the glans penis are complicate presentations in urologic practice. The diseases producing such lesions include psoriasis, Reiter syndrome, lichen planus, lichen nitidus, seborrheic dermatitis, secondary syphilis, fixed drug eruption, erythroplasia of Queyrat, plasma cell balanitis of Zoon, bowenoid papulosis of the genitalia, and discoid and lichenoid chronic dennatosis of Sulzberger and Garbe. The lesions on the glans may not be diagnostic, however, in all of the aforementioned entities except Zoon balanitis, bowenoid papulosis, and erythroplasia of Queyrat, the diagnostic key lies in the examination of the rest of the integument, as the following cases illustrate. [84]
Erosive Lichen Planus Involving the Glans Penis and the oral mucosa may indeed have some histologic similarities, do not believe that the anatomic location alone accounts for the preponderance of plasma cells seen in the biopsy. Lichen planus is generally characterized by a striking absence of plasma cells in the infiltrate. Although scattered plasma cells may be present within the infiltrate of oral lichen planus the predominant cell remains the lymphocyte clearly this is not the case in the report. [2] Found out that in their case the dermal infiltrate was loaded with plasma cells so as to make difficult the differential diagnosis from plasma cell balanitis in the absence of diagnostic epidermal findings. No special significance has been attributed to the presence of many plasma cells in the inflammatory infiltrate occurring within the mucous and semi-mucous membranes. Moreover, it is known that penile semimucous membrane and true mucous membranes share some common characteristics, like parakeratotic keratinization and a lack of cutaneous adnexa, except sebaceous glands. They suggested tliat LP of the glans penis might be similar to LP of the oral mucosa. Since a neoplastic degeneration of the LP affecting the oral mucosa has been documented in 1-9% of the cases, they emphasize the need of a regular follow-up of these eases in order to rule out such a possibility. [2, 44]
Treatment:
Most penile lesions of lichen planus are asymptomatic- If they itch, topical hydrocortisone 0.1 per cent usually provides relief. This disorder is usually self-limited, resolving in a few months. [33]
Lichen nitidus:
Lichen nitidus is an uncommon chronic eruption of tiny skin-colored papules that are usually concentrated on the upper extremities, genitalia, and trunk. The eruption is usually asymptomatic, and the cause unknown. The penis is commonly involved: 9 of 43 cases in a recent series. These tiny papules of lichen nitidus are flesh colored in contrast to lichen planus, winch is violaceous; are not polygonal; and do not usually itch. Other conditions that could be confusing include flat warts, secondary syphilis, sarcoidosis, psoriasis, and folliculitis. Any doubt about the diagnosis can be easily cleared up, as the histopathology of lichen nitidus is distinctive. [94]
Treatment:
Hydrocortisone cream 1 per cent can be applied with fair results- Lichen nitidus. [33]
Lichen sclerosus et atrophicus:
'I his is a descriptive term for a chronic scarring balanitis. Other causes are rare and include pemphigus vulgaris and chronic nonspecific bacterial balanitis. [33]
The association between balanitis xerotica obliterans and lichen sclerosus et atrophicus who described five patients with skin lesions as well as genital involvement. The main symptoms are pain, irritation, disturbance of sexual functions, or urinary symptoms (including obstruction). Rarely tilts can present as a recurrent bullous balanitis, with the development of painful blisters and ulceration which may be precipitated by local trauma. The clinical appearance is of white plaques on the glans, often with involvement of the prepuce which becomes thickened and non-retractile. In active disease haemorrhagic vesicles may be seen. The changes only affect squamous skin, leaving atrophic areas which cause cicatritial shrinkage leading to urethral stenosis and phimosis. [95] The condition affects all ages and circumcision specimens from children with phimosis often show the characteristic histological appearances. Histology initially shows a thickened epidermis, followed by atrophy and foilicular hyperkeratosis. This overlies an area of oedema with loss of the elastic fibers and alteration in the collagen, which in turn overlies a pervascular band of lymphocytic infiltration. Haemorrhagic vesicles occur when the oedema causes detachment of the epidermis with capillary erosion and extravasation of blood. [15] The course is chronic and relapsing, and although it may sometimes arrest, the areas of atrophy do not regress. Development of squamous cell carcinoma has been reported in-patients with balanitis xerotica obliterans, both in areas of active and quiescent disease, but malignant change appears to be less common than in lichen sclerosus et atrophicus in the female. [9] Lichen sclerosus et atrophicus of the penis can cause severe discomfort even without stenosis of the urethral nieatus. A simple operative method is described of removing the involved areas of the glans, the coronal sulcus and the internal surface of the prepuce. A skin flap prepared from the external portion of the prepuce covers the defect. This operation proves to be an effective therapy and gives a good cosmetic and functional result. [75] [83] They are caustically described. First signs of this disease were observed in the age from 3 to 10 years. Compared to 446, 15—81-year-old patient in 161 cases (36%) phimosis was symptom of Lichen planus et atrophicus, too in the same age. [138] In normal skin there was moderate intercellular and intracellular reactivity detected using a high antibody concentration. In specimens with epidermal atrophy they detected intense cytoplasmic and intercellular immunostaming using a lower antibody concentration. The immunoreactivity was independent of the epidermal thickness. Plasma IL-6 measured by radioimmunoassay, was not elevated in plasma from patients with localized or systemic scleioderma. Increased IL-6 in the epidermis of selected skin diseases suggests that 11.-6 may be related to the pathophysiology of dermatologic diseases characterized by epidermal atrophy. [116] Two cases of glans penis epidermoid carcinoma after lichen sclerosus and atrophicus or balanitis xerotica obliterans are discussed. Relationships between both discussed are analyzed but remain not clear. Glans carcinoma can be observed many years later even after circumcision. The knowledge of lichen sclerosus et atrophicus is important to do circumcision at the beginning of the disease with a long-term follow-up of these patients to realize penis biopsy if necessary. Most of lichen sclerosus and atrophicus are not recognized and the frequency would be higher than reported. [49]
Treatment:
Potent Topical steroids usually control the symptoms, although occasionally intralesional steroids may be required. [15] Testosterone ointment has also been advocated. If phimosis is present, circumcision may be required or meatotomy for meatal stenosis. [102] Good hygiene and topical steroids may give temporary, relief. Circumcision will usually cure the problem completely on circumcision. Five patients suffering from a genital or extragenital lichen sclerosus et atrphicus were treated wilh a 2.6% testosterone propionte ointment. An intensive and longer therapy leads to a stop of the illness. The sclerosis itself, however, does not recede. [78] It is therefore necessary to check new methods of treatment. They treated 14 patients with testosterone propionate ointment. In 10 of 14 cases the desired result was achieved. This therapeutic effect was more effective than the results in the control group. [104]
Squamous cell carcinoma:
Squamous cell carcinoma is the most common neoplasm of the penis and is usually located on the glans, prepuce, or coronal sulcus.[108] The ulcerated lesions have a tendency to metastasize earlier. Pain is unusual, although a foul odor and discharge may be present. Phiniosis may be the presenting complaint. [120] Nearly one fourth (23 per cent) of patients will have metastases to the inguinal Lymph nodes at the time of presentation. Sqnamous cell carcinoma carcinoma of the penis is relentless and leads to metastatic disease if not treated. [65] 33-year-old uncircumcised Caucasian male who had a 7-year history of intermittent erosive balanitis and herpes, presented with an 18-month history of progressively worsening penile ulceration not responding to the usual medication. Biopsy of the glans penis carried out in view of the long-standing ulceration showed a sqaumous cell carcinoma of the penis. As there was no response to radiotherapy, partial penectomy was carried out. The importance of early biopsy is emphasized when ulcerative lesions of the penis do not respond adequately to medical therapy. Different treatment modalities available are reviewed. [61]
Thirteen cases of verrucous carcinoma, accounting for 5 per cent of the penile cancers seen during a 25-year interval. Although the typical verrucous pattern predominated minute foci of Invasive squamous carcinoma were identified in 3 patients. All patients were followed for at least 6 years and none has died of the malignancy. Wide surgical excision, usually requiring partial or total penectomy, is the treatment of choice. [88] A guide is presented for nurses to help patients understand and cope with potentially fatal penile cancer. Probably no cancer is more psychologically devastating to a man than cancer of the penis. [71]
Adenosquamous carcinoma of the penis reported with histological evidence of the formation of glandular elements. [85] Neoplasm of the penis is uncommon in the United States, accounting for less than 1 per cent of male cancers. This is thought to be attributable to the high prevalence of circumcision and better hygiene, as penile cancer accounts for as much as 20 per cent of all male cancers in some Third World countries. There may be a history of precancerous lesions such as leukoplakia and lichen sclerosis et atrophicus (balanitis xerotica obliterans). [120] The most common penile neoplasm is Squamous cell carcinoma, but there are also occasional basal cell carcinomas, malignant melanomas, and sarcomas. [65] The major problem in these neoplasms is the reluctance of the patients to come forward for treatment. One study found that most patients had delayed seeking care for more than a year and that 17 per cent had come in only after sloughing off a significant portion of the penis-The presenting complaint in some patients will be lumps in the groin from metastatic disease. [65]
Treatment:
Historically, treatment has been partial amputation with a 2-cm proximalmargin tumor on the glans and distal shaft. Total penectomy is performed for larger lesions. [21,103] Controversy still exists over the need for a prophylactic inguinal lymphadeneclomy. Biopsy of a "sentinel" node located at the juncture of the saphenous and femoral veins for staging purposes seems reasonable. [23] The cosmetic and functional outcome of laser treatment for stages Tis to 1 T2NONo, grades 1 and 2 squamous cell carcinoma of the penis is excellent, and the associated morbidity rate is low. [137] If microinvasion through the basal layer of the epidermis has occurred, the lesion should be treated as squamous cell carcinoma. Approximately 5 per cent of Bowen's disease cases have metastasized at the time of diagnosis despite, the inability to document microinvasion. These lesions are sometimes considered "precancerous" and have been treated with liquid nitrogen or topical 5-Fuorouracil.They are probably best locally excised, however, since the carcinoma in situ in these lesions tracks down the hair follicles, where it is difficult for topical or cryotherapy to reach. Mobs' micrographic surgery may spare tissue and given higher cure rates. [21] Lymph node biopsy is probably not indicated. Some authors would recommend a limited search for an internal malignancy including a chest roentgenogram, upper and lower gastrointestinal series, and intravenous urogram if the Bowen's disease occurs on a nonsun-exposed area. [103]
Patients and Methods:
Study area:
This study was performed in Al-Kuwait University Hospital, which lies in the west zone of Sana'a city near Sana'a University. It contains 200 beds for all brandies of medicine, except dermatology, which has an Out- patient Dermatology Department (D.O.P.D.). In addition, there is main laboratory for the of Hematology, Microbiology, Pathology and Serology investigations.
Study populations:
One hundred and fifty-one circumcised Yemeni male patients ranging from 6 to 60 years with balanitis were classified into three groups:
9 cases were presented with irritant balanitis, 131 cases with infective balanitis and 11 cases with other chronic unresolving conditions of balanitis. Most Yemeni people who work in agriculture as fanners they live in small and big houses in the of mountains tops, in vallies and the coast of the red and Arabic sea. Most of those houses are built of stones. They depend in their live on the rain and ground water supply for their livelihood and therefore the poor hygiene is high.
Study design:
Balanitis is an acute or chronic inflammation of the glans penis "Posthitis" refers to an inflammation of the mucous surface of the prepuce. The term balanoposthitis thus refers to an inflammation of the penile skin. This study used the descriptive prospective method. The simple size were 151 cases out of 26324 dermatological cases presented in Al-Kuwait University Hospital (Sana'a) since 1996 till 1998.9, 131 ,11 cases were screened as irritant, infective and oilier chronic unresolving conditions of balanitis respectively. One hundred and thirty-one cases of infective balanitis; 50 cases manifested with burning and itching of the penis with generalized erythema of the glans, which may have a dry glazed appearance, with eroded white papules and white discharge. In 50 cases the penile lesions were small erythematous, sometimes coppery or bronzed, slightly hyperkeratotic, papules that itchy severely. In 18 cases manifested with not itchy erythema and multiple pustules covering with crusts. In 13 cases manifested with patchy or small warty lesions in the glans penis. Vesicles and umblicated pearly papules with fever and chils were noted. In 11 cases of other chronic unresolving conditions of balanitis manifested with erosive non-itchy plagues covered with white scales, small brownish skin colors papulo-vesicular eruptions and large eroded ulcer of all the glans penis.
Tools and Instruments:
Myocology:
Skin scraping is a simple method for investigation of penile skin lesions by using the scalpel to scrap the skin lesions of the glans penis. It was tested for superficial dermatophytosis (fungi), candidiasis and scabies by addition a drops of potassium hydroxide (KOH 10-20%). Left in the glass slide for 20 minute and examined on the light microscope and in addition of the germ tube test and sabroud agar medium and KOH 10-20% used also in the examination of 50 cases. The wood's light used to detect the color of the skin lesions of those cases.
Stool and Urine analysis were performed in all the 151 cases. The intestinal protozoa (Entameba histolytica) were demonstrated in the most of 151 study populations.
Serology Serological tests for syphilis, either non-specific (Wassermann and venereal disease reagent level) or specific (Treponema pallidum hemoaggulatination test) were done for the 151 cases. The serum blood level for random and fasting blood sugar and serological tests for HIV (Enzyme Linked Immune Sorbet Assay ELISA, and Western blotting technique) was performed.
Microbiology Skin swab from the discharge or pus of the glans penis skin lesions, spreading in the glass slide, staining with Gram-ve and Gram+ve staining and cultured in blood agar midium and Mackonky medium in 16 cases. The therapeutic modalities topical and systemic of antifungals, antipruritic, antibiotics, antiscabietic, antiviral, corticosteriod and chemical and electrical cauterarizalion were done.
Pathology Skin biopsies were done by shaving, elliptical incision and punch biopsy methods. The specimens were put in a bottle filled with 20% formaline and sent to the pathological laboratory to be stained with Hematoxylin and Eosin. The sections in slides for all the 151 cases were examined under the light microscope. The special stains were not indicated, and the Hematoxylin and Eosin is enough for staining.
Results:
Table 1 shows the characteristics of study populations 151 cases of balanitis. Histopathological findings of 9 cases of irritant balanitis were nonspecific, mild dermal perivascular infiltrate and spongiosis of the epidermis. 131 cases of infective balanitis 50 cases of post scabietic papules with pseudoepithilomatous hyperplasia, hyperkratosis, dermal pigmentary incontenence and perivascular lymphohhisteocytic infiltrate. The female mites were absent. 50 cases were candidiasis with mild dermal perivascular infilammatory infiltrate and 13 cases of epidermal and dermal viral reaction. Eleven cases of other chronic conditions of balanitis with psoriasifonn appearance, lichenoid reaction and mitotic figures appearance. Skin scraping in 50 cases of balanitis candidiasis revealed the presence of hyphae and spores in addition Sab. Agar medium culture and germ tube test were positive. The blood sugar, Wood's light, serological tests for syphilis and HIV with no abnormal detection. Gram+positive staining showed staphylococcos aureus balanitis in 2 cases, Gram-ve staining was positive with GBBHT balanitis in 14 cases and the blood agar medium was positive. Stool and urine analysis were normal, Tzanck test revealed in 7 cases of herpes simplex progenitalis balanitis. The poor hygiene was high especially in the married males with candidal and scabietic balanitis.This means the high incidence of balanitis in with those two diseases.
Table 2 shows 9 cases of irritant balanitis 5.95%, 5 cases of contact dermatitis 3.31% due to masturbating manually with soap, fixed drug eruptions with sulpha (septrin) in 2 cases 1.32%, metroniadazole in 1 case 0.66% and Ampicillin in 1 case 0.66%.
Table 3 shows 131 cases of infective balanitis 85.62%, scabietic in 50 cases of married males 33.11%, candidal in 50 cases of married males 33.11%, Group B Beta Flemolytic Streptococcos in 16 cases 10.59%, Staphylococcos aureus in 2 cases 1.32%, human papilloma virus in 2 cases1.32%, herpes simplex progenitalis in 7 cases 4.63%, and mollusum contagoisum in 4 cases 2.64%.
Table 4 shows 11 cases of the other chronic conditions of balanitis 7.27%, psoriasis in 5 cases 3.31%, lichen planus in 3 cases 1.98%, lichen nitidus in 1 case 0.66%, lichen sclerosus et atrophicus in 1 case 0.66%and squemaous cell carcinoma in 1 case 0.66%. The data analysis in the Tables 1, 2,3,4, was done manually while the data was reported.
|
Investigations |
Irrit.B(n =9) |
lnfec.B(n=13l) |
O. Ch. Unres. Cond. B.(n=11) |
|
Skin biopsy |
Non-Specific |
Non-Specific |
Non-Specific |
|
Skin scraping |
-ve |
Spores + hyphae in 50 cases |
-ve
|
|
Sabouraud agar media |
-ve |
+ve |
-ve
|
|
Germ tube test |
-ve |
Specific in 50 cases of Candidiasis |
-ve |
|
Wood's light |
-ve |
-ve |
-ve |
|
Blood sugar |
|
-ve |
-ve |
|
Serological tests for Syphilis. |
-ve |
-ve |
-ve |
|
Serological tests for HIV |
-ve |
-ve |
-ve |
|
Gram-positive Staining |
-ve |
Staph.Aureus in 2 cases |
-ve |
|
Gram-negative Staining |
-ve |
GBBHT in 14 cases |
-ve |
|
Blood Agar Media |
-ve |
GBBHT in 14 cases |
-ve |
|
Stool analysis |
-ve |
-ve |
-ve |
|
Urine analysis |
-ve |
-ve |
-ve |
|
Poor hygiene |
-ve |
+ve |
-ve |
|
Tzenck |
-ve |
+ve in 7 cases |
-ve |
Table 1: Characteristics of study populations
|
Irritant Balanitis |
Cases (N=151) |
Percent |
|
Contact Dermatitis - Masturbation manually with soap |
5 |
3.31%
|
|
Fixed drug eruptions Sulpha (Septrin) Metronidazole Ampicillin |
2 1 1 |
1.32% 0.66% 0,66% |
Total 9 5,95%
Table 2: numbers of irritant balanitis cases
|
Infective Balanitis |
Cases (N-l 51) |
Percent |
|
Parasitic - Scabietic |
50 |
33.11% |
|
Candidal |
50 |
33.11%
|
|
Bacterial - GBBHS - Staphylococcus aureus |
16 2 |
10.59% 1.32% |
|
Viral -HPV -Herpes simplex progenitalis -Molluscum contagiosum |
2 7
4 |
1.32% 4.63%
2.64% |
Total= 131 85.62%
Table 3: numbers of infective balanitis cases
|
Other chronic conditions of Balanitis |
Cases (N=151) |
Percent
|
|
Papulosquamous eruptions Psoriasis Lichen planus Lichen nitidius Lichen sclerosous et atrophicus
|
5 3 1 1 |
3.31% 1.98% 0.66% 0.66%
|
|
Malignant - Squamous cell carcinoma |
1 |
0.66%
|
Total= 11 7.27%
Table 4: numbers of other chronic unreslving cases of balanitis

Figure a: balanitis due to scabies female mites
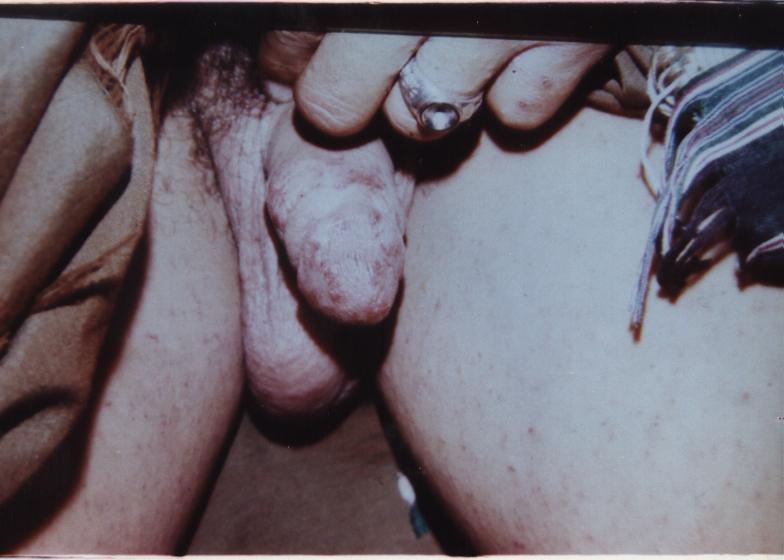
Figure b: balanitis due to scabies female mites.

Figure c: balanitis cutaneous candida albicans yeasts.

Figure d: balanitis due to cutaneous candida albicans yeasts.

Figure e: balanitis due to Staphylococcal aureus bacterial organism.

Figure f: balanitis due to Beta heamolytic streptococcal bacterial organism.

Figure g: balanitis due to Human papilloma Virus (genital wart)
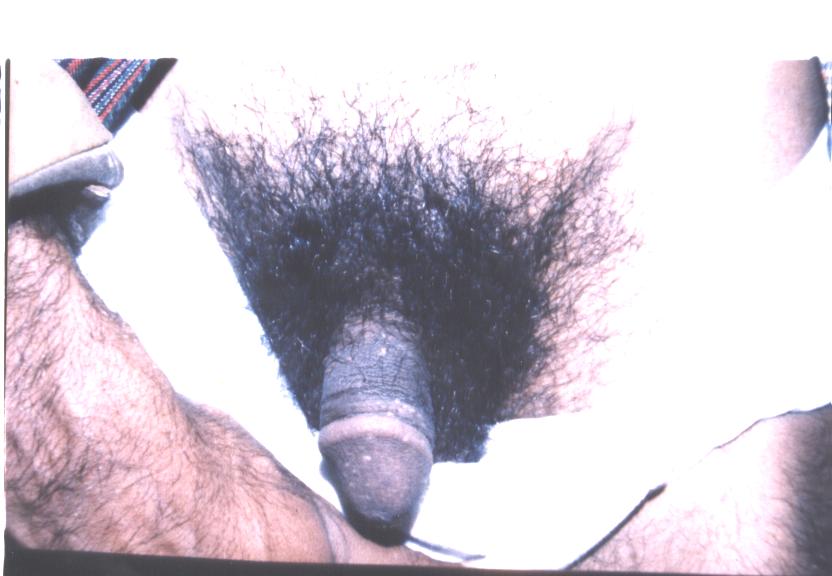
Figure h: balanitis due to Molloscum contagiosum virus

Figure i: balanitis due to Herpes simplex type 2 progenitalis virus.
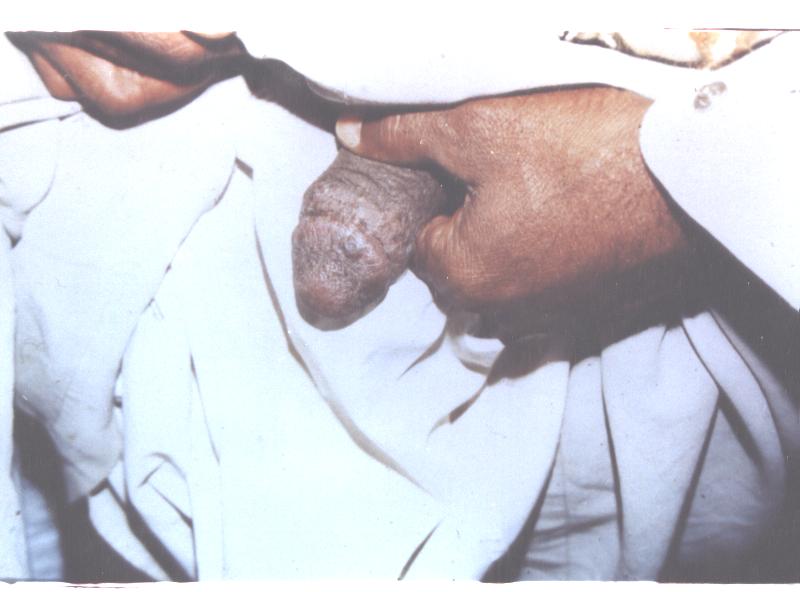
Figure j: balanitis due to Herpes simplex type 2 progenitalis virus.

Figure k: balanitis due to Fixed drug eruption from sulphamethoxazole.

Figure l: balanitis due to fixed drug eruption from Ampicillin

Figure m: balanitis due to fixed drug eruption from Metronidazole
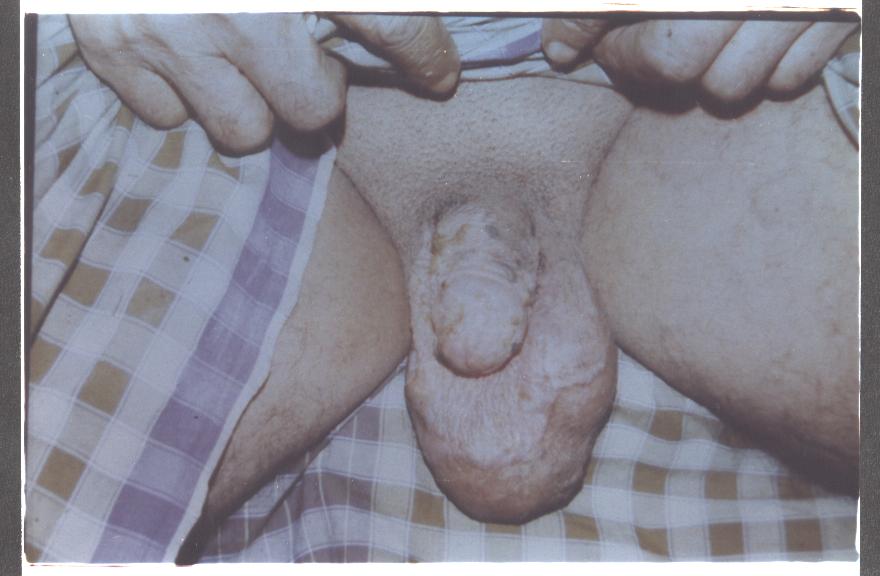
Figure n: balanitis due to erosive chronic lichen planus.

Figure o: balanitis due to lichen sclerosus et atrophicus

Figure p: balanitis due to lichen nitidus.

Figure q: balanitis due to erosive chronic psoriasis.

Figure r: balanitis due to Ulcerative and Eroded type of squamous cell carcinoma of the glans penis
Discussion:
Irritant and allergic balanitis:
Many cases of men balanitis studied. [10] They regarded that these are often due to irritation, particularly if symptoms are persistent or recurrent. In one study of patients with persistent or recurrent problems 72% were diagnosed are irritant balanitis, and this was associated with a history of atopy and more frequent genital washing with soap. But others [1, 6, 74,130] had found higher rates of infective agents; although a large proportion of cases in one study remained undiagnosed. It is likely that [34, 52] study in which the irritation plays some part in other balanitides. More severe reactions have been seen with topical agents, some of which may have been used for treatment. Dequalinium is known to cause a necrotic balanitis, while titanium (that was previously thought to be biologically inert) may rarely cause a granulomatous balanitis. On the other study of [81,128] the balanitis as an allergic reaction is very uncommon; rubber and its constituents are the most frequently described allergens, although allergy to spermicidal lubricants are also well described. The demonstration of [110] proved that the striking more numerous quote of balanitis in mental retarded boys is diseased due to sexual hygiene, the cleanness of the hands while miction of man, about the cleanness of the inferior abdomen, the cleanness of pants and the hygiene of the toilet. It is clear from the previous studies [54, 34] that the washing of genitalia with soap, rubber, lubricants spermicidal, sexual hygiene and topical agents were the causes of irritant balanitis, and the clinical manifestations varying from balanitis to oedema of the whole penis extending to the groins. This confirms the study in this hypothesis. In this study the antimicrobial drugs as ampicillin, sulphamethoxazole trimethoprime and metronidazole caused allergic irritant balanitis (fixed drug eruptions) with well-defined erythema and violaceous plaque in the glans penis. Fixed drug eruptions have a predilection for the glans penis, and are commonly related to therapy with, antibiotics especially tetracycline and sulphonamides. But the other causes include salicyclates, phenacetin, phenolphthalein and some hypnotics, although there are case reports of other less common causative agents. However, tetracycline induced eruptions. The other studies regarded the lesions are usually well demarcated erytlicmatous areas which may be bullous and subsequently ulcerated. This can occur on the first exposure to a drug and repeated exposure will precipitate new lesions at (lie initial site (tins can confirm the diagnosis. Most lesions will fade spontaneously without treatment but may leave an area of residual hyperpigmentation. Occasionally treatment with topical, or rarely, systemic steroids may be required. [36, 37, 21, 6, 46, 74]
Infective Balanitis:
Scabies and candida balanitis were common in the married males than the singles males due to the high incidence of poor or sexual hygiene and the two conditions transmitted by sexual contact between the two partner's husband and his wife. The other causes were Group B beta haemolytic streptococcus (erythema, vesicle, and crust), staphylococcus aureus (pastilles), human papilloma virus (genital wart), recurrent herpes simplex progenitalis (vesicles) and molluscom contagiosum (pearly hemispherical umblicated papules). However, scabietic balanitis in their studies and they considered scabies infestations rarely involve the penis alone, and the patient will usually volunteer that he is itching mightily. [22, 33, 64, 86] Men usually have penile lesions, and these are small erythematous, sometimes coppery or bronzed, slightly hyperkeratotic, papules that itch severely. But Candidal balanitis to be the most common cause of balanitis and is due to infection with candidal species, usually Candida albicans. It is generally sexually acquired although, carriage of yeasts on the penis common, being 14-18% with no significant differences between carriages retain circumcised or uncircumcised men. Symptomatic infection is more common in the uncircumcised male. Significantly more of the female partners of men carrying yeasts were found to have candidal infection. Diagnosis may be on the clinical appearances alone, microscopy and/or culture. The sensitivity of microscopy varies with method of sampling, and an "adhesive tape" method has proven to be more accurate than swabbing. Infection may occur without sexual contact, usually in the presence of diabetes of which it may be the presenting symptom or after the use of oral antibiotics. Symptoms are of burning and itching of the penis with generalized erythema of the glans and/or prepuce which may have a dry glazed appearance, with eroded white papules and white discharge. [39, 115, 45, 135, 74, 6] Group B streptococci can be carried asymptomatically in the adult genital tract, but strongly associated with balanitis. Rate of carriage varies between heterosexuals and homosexuals (16.6% in heterosexuals and 39.3% in homosexuals) although no balanitis occurred in the latter group. Sexual transmission is unclear as there was no expected age differential in one study, and in another meatal carriage was not proportional to promiscuity. The clinical appearance is of nonspecific erythema with or without exudate, but more rarely may extend to penile cellulitis if abrasions are present Staphyloccocus aureus has infrequently been reported as causing a balanitis, although carriage is not strongly associated with symptoms. [8, 17, 132, 97, 50, 1,107] rare cases of primary herpes can cause a necrotising balanitis, with necrotic areas on the glans accompanied by vesicles elsewhere and associated with headache and malaise. This has been reported with herpes simplex virus types I and 2. But the Papillomavirus may be associated with a patchy or chronic balanitis, which becomes acetowhite after the application of 5% acetic acid. Acetowhite change has also been reported in non-HPV associated balanitis and has resolved on treatment. While molluscum conlagiosum lesions may be found on the penis or the perigenital area a usually spread by sexual contact in adults. From the above- mentioned studies the scabictic and candidal balanitis were common while the HPV, herpes simplex progenitalis and mollusciun contagiosum lesions in the glans penis were rare. [109, 4, 11, 72,136]
Other chronic unresolving conditions of balanitis:
In this study the other chronic unresolving conditions causes balanitis were psoriasis (red plaques not covered by silvery scales), erosive lichen planus (itchy violaceious flat papules), lichen nitidus (small glisning papules) and lichen sclerosus ET atrophicus (haemorrhagic vesiculo-papular skin lesions in the glans penis). Squamous cell carcinoma manifested by severe ulceration of the glans penis without secondaries to the regional lymph nodes. Psoriasis commonly occurs on the penis, and occasionally the penis is the only site affected. The preputial glans is the most common site involved. Red plaques with well-demarcated borders and a dull, velvety, granular surface are seen. Often, there is a red ring of involvement around the edge of the glans. The silvery scale commonly associated with psoriasis is usually not seen on the glans, particularly in the uncircumcised. Psoriasis in the shaft will have silver or amber scale. The most important diagnostic clue or psoriasis is a history or presence of lesions elsewhere. The differential diagnosis for penile psoriasis includes balanitis circinata (Reiter's syndrome), plasma-cell balanitis, erythroplasia of Queyrat and Bowen's disease, bowenoid papulosis, lichen planus, and fixed drug eruption .They added that the Lichen planus is usually, involve of the penis in 25 per cent of cases in males. Often, there are lacy reticulate lines on the buccal mucosa that aid in diagnosis. Penile lesions, in the absence of papules elsewhere, are rare. There are usually many, tiny, shiny, polygonal papules on the glans that can be difficult to tell from lichen nitidus. [33, 86] Lichen nitidus is commonly involving the penis. Lichen scierosus et atrophicus described in five patients with skin lesions as well as genital involvement in the glans penis. the clinical appearance is of white plaques on the glans, often with involvement of the prepuce which becomes thickened and non-retractile. In active disease haemorrhagic vesicles may be seen and the condition affects all ages. Squamous cell carcinoma is by far the most common neoplasm of the penis and is usually located on the glans, prepuce, or coronal sulcus. Pain is unusual, although a foul odor and discharge may be present. Phimosis may be the presenting complaint. Nearly one fourth (23 per cent) of patients will have metastases to the inguinal Lymph nodes at the time of presentation. Squamous cell carcinoma of the penis is relentless and leads to metastatic disease if not treated.
It is obvious from the previous studies the other chronic unresolving conditions of balanitis were rare and therefore confirmed this study. [94, 95, 108, 120, 65]














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org