Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Humberto Morais1*, Valdano Manuel2,3
1Department of Cardiology Hospital Militar Principal/Instituto Superior, Luanda, República de Angola.
2Division Cardiovascular Surgery. Universidade de São Paulo, Hospital das Clínicas da Faculdade de Medicina, Heart Institute, São Paulo, SP, Brazil.
3Cardio-Thoracic Center, Clínica Girassol. Luanda, República de Angola.
*Corresponding author: Humberto Morais, Hospital Militar Principal/Instituto Superior Rua Pedro Miranda 40-42 Maianga Luanda República de Angola
Received: May 31, 2021
Accepted: June 04, 2021
Published: June 6, 2021
Citation: Morais H, Manuel V. “Hepatocellular Carcinoma Diagnosed by Tumor Thrombus in The Right Atrium”. Clinical Case Reports and Clinical Study, 4(3); DOI: 10.61148/2766-8614/JCCRCS/073
Copyright: © 2021 Humberto Morais. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
We report the images of an octogenarian female patient admitted to the hospital with complaints of dyspnea, melena, and ascites in which the diagnosis of hepatocellular carcinoma with tumoral thrombi invasion of the portal vein, the hepatic veins, the inferior vena cava, and the right atrium was made. Regarding the case, the authors make a brief review of the literature on the diagnostic and therapeutic approach of these patients.
Case report
We report the images of an octogenarian female patient admitted to the hospital with complaints of dyspnea, melena, and ascites. Her medical history included systemic arterial hypertension, hepatitis-B-virus infection, and chronic liver disease. The transthoracic echocardiogram showed a large mass in the right atrium (figure 1 A and B).

Figure 1: Transthoracic echocardiogram A - parasternal long axis view for the right chambers; B - apical view four chamber view showed a large mass in to the right atrium, (blue arrow).
The thoracic and abdominal computed tomography (CT) scan confirmed an image of a soft tissue mass in the hepatic vein, inferior vena cava, and right atrium, which was consistent with a tumor thrombus (figures 2 A and B), and showed also the liver with irregular contours and a hypodense lesion in the right lobe measuring 5.9 × 5.6 cm in its longest axis, consistent with hepatocellular carcinoma figure (2C and D). Voluminous ascites and portal vein thrombosis were also present.
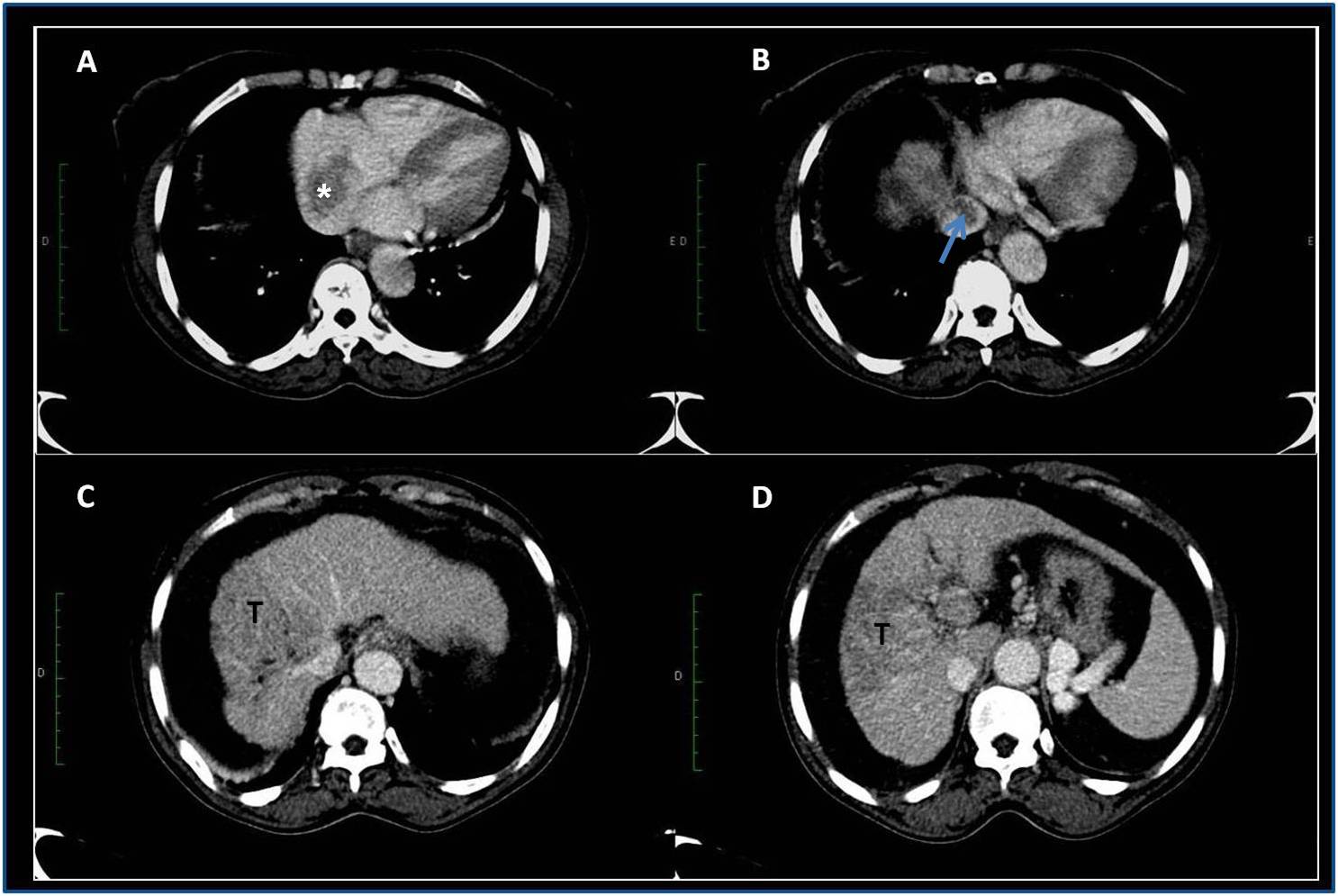
Figure 2: A – Cardiac computed tomography showing a large mass in to the right atrium, star. B - Inferior vena cava filled with thrombus, arrow. C and D – Abdominal computed tomography showing the liver with irregular contours, hypo-dense lesion in the right lobe measuring 5,9 x 5,6 cm in the largest axis. T- tumor.
The patient was hospitalized in the intensive care unit. Surgery was contraindicated due to clinical instability facing a high-risk procedure. She died 25 days after admission. The autopsy confirmed the CT findings. The histological report rendered the diagnosis of poorly differentiated HCC (grade IV) in the liver, and a tumoral-thrombi of the portal vein, the hepatic veins, the inferior vena cava, and the right atrium.
Discussion
Hepatocellular carcinoma (HCC) is a highly aggressive and invasive cancer of the liver. HCC is one of the most common cancers in adults and is the third cause of cancer-related mortality worldwide. (1,2) Cirrhosis, usually of the micronodular type, was found in 72% of 490 autopsied cases of HCC. (3) Similarly, the association with chronic hepatitis B and C infections is frequently found in HCC cases. (1) The increasing hepatitis C infections have tripled the age-adjusted incidence rate of primary liver cancer in the USA. (4) Advanced-stage HCC usually metastasizes to the lymph nodes, lung, bone, brain, and adrenal glands. (2) Moreover, tumor growth in the vascular system is well documented. The incidence of HCC with direct invasion to the heart is 1% to 4%.(2,5 ). However, the antemortem diagnosis of cardiac involvement is not easy nor is it frequent.(6) Microscopic vascular invasion at diagnosis is seen in 60% to 90% of patients with HCC greater than 5 cm.(2-6) In large autopsy series, the extension of HCC to the portal and hepatic veins occurred in 29% to 65% and 12% to 54%, respectively.(3,7,8) The involvement of the hepatic veins extends to the inferior vena cava and reaches the right atrium and right ventricle favoring embolization.(9) However, synchronous invasion of the heart and the portal veins has been scarcely reported.(5)
Patients with HCC with an invasion of the vascular bed have a guarded prognosis.(5,6) Surgical resection, liver transplantation, transarterial chemoembolization, and systemic chemotherapy are therapeutic options in selected cases of HCC.(1,2,5,6) Despite these interventions, the median survival ranges between 2 and 20 months.(1,2,5) Importantly, a tumor thrombus, defined as a tumor extending into a vessel (typically a vein) or in the right atrium, can be overlooked or interpreted as a simple right atrium thrombus. The differential diagnosis between metastases and other cardiac masses is therefore of paramount importance.(10).
The patient was hospitalized in the intensive care unit. Surgery was contraindicated due to clinical instability facing a high-risk procedure. She died 25 days after admission. The autopsy confirmed the CT findings. The histological report rendered the diagnosis of poorly differentiated HCC (grade IV) in the liver, and a tumoral-thrombi of the portal vein, the hepatic veins, the inferior vena cava, and the right atrium.
Conflicts of interest: None declared
Funding: None














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org