Clinical Case Reports and Clinical Study
OPEN ACCESS | Volume 13 - Issue 1 - 2026
ISSN No: 2766-8614 | Journal DOI: 10.61148/2766-8614/JCCRCS


Ibrahim Farah1, Ali Abdelghaffar3, Hanaa Elmahdy2, Yasser Mubarak4
1Consultant Cardiac Surgery, Madinah Cardiac Center, Medina, KSA.
Lietenden Oberaztes fur Herz – und thoracchirurgie Klinikum Krefeld Germany
2Cardiology Consultant at Cardiology Departments at King Fahad Hospital, Medina, KSA.
3 Cardiology Registrar at Cardiology Departments at King Fahad Hospital, Medina, KSA.
4 Assistant Professor of Cardiothoracic Surgery, Minia University, Egypt. Associated Consultant of Cardiac Surgery, Madinah Cardiac Center, Medina, KSA.
*Corresponding author: Yasser Shaban Mubarak, MD. Assistant Professor of Cardiothoracic Surgery Department, Faculty of Medicine at Minia University.
Received: March 15, 2021
Accepted: March 22, 2021
Published: March 26, 2021
Citation: Ibrahim Farah, Ali Abdelghaffar, Hanaa Elmahdy, Yasser Mubarak. “Acute Severe Mitral Regurgitation due to Papillary Muscle Rupture after Blunt Chest Trauma: Case Report”. Clinical Case Reports and Clinical Study, 3(1); DOI: 10.61148/2766-8614/JCCRCS/039
Copyright: © 2021 Yasser Shaban Mubarak. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cardiac injury is a common unexpected organ injuries leading to mortality in polytrauma patients. Cardiac injuries following blunt chest trauma vary from myocardial contusions to fatal rupture. (Shaikh N., et al. 2013)
Blunt cardiac injury is about 15—25% of blunt chest trauma. The most common form is cardiac contusion with variable manifestations accompanied by electrocardiogram (ECG) or cardiac enzyme abnormality. (Yang S., et al. 2011)
Traumatic rupture of intra-cardiac structures is an uncommon after blunt chest trauma; however there are few reports related to rupture of intra-cardiac valves. Valves involvement are uncommon, the most frequent being the aortic valve, followed by the mitral and tricuspid. Nowadays, there has been a rise in the incidence of these injuries due to increase of road traffic accidents (RTA). (Bernabeu E., et al. 2004)
Rupture of papillary muscle or its chordae tendineae following blunt chest trauma is a very rare causing acute mitral insufficiency with subsequent congestive heart failure (HF) and pulmonary edema. (Shaikh N., et al. 2013)
Introduction
Blunt chest trauma seldom results in cardiac injury, which varies in severity from asymptomatic myocardial contusion to fatal cardiac rupture (Cresce GD., et al. 2009). However, intra-cardiac injury incidence has been described aortic then mitral regurgitation seems to be extremely rare (Bernabeu E., et al. 2004). Blunt chest trauma is a rare cause of acute mitral regurgitation (MR). Papillary muscle rupture caused by blunt chest trauma is a relatively rare cause of mitral incompetence (Simmers T., et al. 2001) (Cresce GD., et al. 2009).
The mechanisms of injury could be the sudden increase of intra-ventricular pressure due to compression of the heart between sternum and vertebral column, or due to the sudden deceleration injury with the heart being pushed forward against the sternum (Cresce GD., et al. 2009). Sudden deceleration or compression of the heart with subsequent damage to the closed atrioventricular valve or subvalvular apparatus is responsible; patients are generally road traffic accident (RTA) victims (Simmers T., et al. 2001).
Traumatic mitral valve (MV) injury occurs during late diastole and early systole. The most common mitral injury is papillary muscles rupture, followed by the chordae tendineae, and a leaflet tear. Manifestations of traumatic mitral injury include a wide range of presentation varying from asymptomatic to acute cardiogenic shock. (Bernabeu E., et al. 2004)
Case report
We report a case of 27-year-old male patient with no previous medical diseases. He was complaining of shortness of breath (SOB) and stitching chest pain after road traffic accident (RTA) one week ago. His vital signs were Heart Rate 100 beats/minutes (tachycardic), Blood Pressure 100/70 mmHg, Respiratory Rate 35 breath/minute (tachypneic), Temperature 36.5°c, Glasgow Coma Score (GCS) 14/15, and O2 saturation 94% on 3Liters breath mask. On auscultation a significant pansystolic murmur was heard at apex propagated to axilla. Electrocardiography (ECG) revealed diffuse ST concave elevation. Laboratory data was Troponin I (0.011 ng/ml), lactate dehydrogenase (LDH) (1,54 mU/mL) and creatine phosphokinase (CK) (456 mU/mL). Arterial blood gas (ABG) analysis in a 3Liters breath mask were as follows: pH 7.35, carbon dioxide tension 42.5 mmHg, oxygen tension 84 mmHg, base excess of –2.0 mmol/L and oxygen saturation 94%. Chest X-ray showed diffuse opacity patches bilaterally without thoracic cage fracture or pneumothorax or pleural effusion. Chest computed tomography (CT) revealed bilateral infiltration. Covid-19 swab was done and result was negative. Transthoracic echography (TTE) revealed severe mitral regurgitation with fail anterior mitral leaflet and rupture of anterolateral papillary muscle (Figure 1,2). EF was 77%. Within twelve hours of admission to emergency department, he developed progressive worsening SOB and was transferred to intensive care unit (ICU), where he received intravenous Furosemide and Nitroglycerin. Final diagnosis was traumatic rupture of anterolateral papillary muscle of MV, after blunt chest trauma, causing acute severe MR and pulmonary edema. He accepted surgery and transferred to cardiac surgery center. Then, emergency mitral valve replacement performed.

Figure (1):- TTE revealed severe mitral insufficiency with rupture papillary muscle

Figure 2: TTE revealed flail anterior mitral valve leaflet
The decision was made to operate, with the intention of repairing the valve, if possible. After induction, TEE was performed, confirming severe MR, together with an echogenic mass prolapsing into the left atrium (LA). This mass was presumed to be the papillary muscle (PM). After the institution of cardiopulmonary bypass (CPB) and cardioplegic arrest, LA was opened. The anterolateral PM had torn out of the left ventricular wall and twisted itself several times around the chordae. Because of the possibility of failure with simple re-attachment of the anterolateral PM to the friable ventricular wall, the MV was replaced with St. Jude Medical 29-mm mechanical valve (Figure 3). The atrium was closed, and the patient weaned off bypass easily. His postoperative course was uneventful, and an echocardiogram on the 5th postoperative day (POD) showed well function prosthetic MV with good EF. He was discharged to home the 10th POD after INR adjusted, and was seen in clinic 2 weeks later, at which time he was asymptomatic. 3-month follow-up period, clinical was well and asymptomatic, TTE revealed well function MV without gradient, and INR was 2.5 on warfarin 5mg.
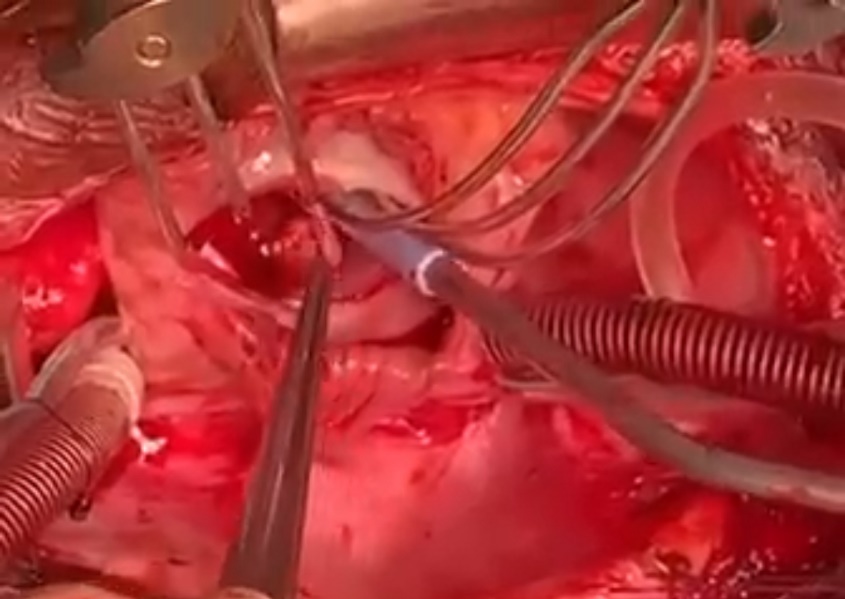
Figure 3: intra-operative photo of rupture papillary muscle
Discussion
Thoracic trauma is a common reason for presentation to the emergency services, especially following RTA. Myocardial contusion is frequent sequelae. However, acute valvular dysfunction following blunt chest trauma is a rare event (Halstead J., et al. 2000). First mitral traumatic rupture was reported in 1936 and the first successful repair in 1964 (McLaughlin JS., et al. 1964). Recently, the incidence of blunt chest trauma has been increasing because of traffic accidents, and a few cases unfortunately lead to death without appropriate diagnosis and treatment in spite of improved diagnostic procedures and surgical techniques due to lack of high index of suspicion. Generally, myocardial injuries are not uncommon, although MV injury is very rare. In cases of blunt chest trauma, it is clinically important to detect new systolic murmurs and any symptoms of heart failure (HF), and to do urgent surgery. Ordinarily, TTE and TEE are used as diagnostic tests for this injury. Surgeons should determine whether to perform MV repair or replacement according to intraoperative findings. Mitral Valve Replacement (MVR) is a reliable and simple procedure. The choice for a particular approach must be based on the extent of damage, accurate analysis of the mitral apparatus and surgeon’s technical expertise (Bernabeu E., et al. 2004).
Traumatic acute severe MR is thought to occur as a result of loss of valve integrity from a sudden increase in intra-cardiac pressure while the heart is completing diastole and entering systole, with the ventricles dilated and the atrio-ventricular valves closed. Most frequently damaged is the papillary muscle, followed by the chordae tendineae. Symptoms of acute MR are due increased LA pressure and decreased left ventricular EF. Acutely, the patient usually presents with signs of pulmonary edema such as dyspnea, cough and orthopnea (Petteys S., et al. 2011).
Blunt injury to the cardiac valves leads to progressive HF often requiring surgery. Most frequently, prosthetic replacement is the option of choice. MR following non-penetrating cardiac injury is usually the result of PM rupture, other causes being chordal rupture, or leaflet disruption. Papillary rupture can be partial occurring through one of the heads, or complete through the muscle body. In this latter case especially, severe left ventricular failure ensues and surgical management is usually essential. The presentation can be delayed, perhaps due to eventual rupture of a necrotic papillary muscle contused in the initial trauma (Halstead J., et al. 2000).
Cardiac valve injury is an uncommon clinical entity, the recognition of which is difficult at the time of initial evaluation in cases of blunt chest trauma. Because the patient with traumatic valve injury often has hemodynamic instability, insufficient visualization of the friable endocardium, and necrotic PM, the valve repair is neither easy nor safe. Especially for MV, some authors have recommended that valve replacement should be done for all cases of acute valvular disruption. A high index of suspicion is important for the early diagnosis of traumatic valve injury. Even when cardiac valve injury is equivocal, one should not hesitate to perform TEE (Choi JS, and Kim EJ. 2008).
Traumatic MR if not detected early and treated properly can get complicated and progress to congestive HF and cardiogenic shock. This primary damage resulted in the development of coagulation necrosis, resulting in subsequent rupture. Patient’s clinical condition will detect the timing and type of surgery (Shaikh N., 2013).
Conclusion
In cases of blunt chest trauma, it is clinically important to detect newly developed systolic murmurs and any symptoms of congestive heart failure. Echography is essential in diagnosis. It is important to perform surgery in a timely fashion. Replacement of injured mitral valve is safe, rapid, and the suitable option in most cases.
Abbreviations
ABG: arterial blood gas, CK: creatinine kinase, CPB: cardiopulmonary bypass, CT: computed tomography, ECG: electrocardiography, EF: ejection fraction, GCS: Glasgow coma score, HF: heart failure, INR: international normalized ratio, LA: left atrium, LDH: lactate dehydrogenase, MR: mitral regurgitation, MV: mitral valve, MVR: mitral valve replacement, SOB: shortness of breath, PM: papillary muscle, POD: post-operative day, RTA: road traffic accident, TEE: trans-esophageal echo, TTE: trans- thoracic echo.














Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org