Aditum Journal of Clinical and Biomedical Research
OPEN ACCESS | Volume 8 - Issue 1 - 2026
ISSN No: 2993-9968 | Journal DOI: 10.61148/2993-9968/AJCBR


Malik Shahnaz 1, Snober Malik 2, Amat us Sami 3*, Sheeba Altaf 4 and Naveed Bashir 5
1Consultant Surgeon, Directorate of Health Services, Kashmir
2Consultant Gynaecologist, Directorate of Health Services, Kashmir
3Consultant Surgeon, Directorate of Health Services, Kashmir
4Medical officer, Directorate of Health Services, Kashmir
5Consultant Orthopaedician , Directorate of Health Services, Kashmir
*Corresponding Author: Amat us Sami, Consultant Surgeon, Directorate of Health Services, Kashmir.
Received Date: July 13, 2022
Accepted Date: July 14, 2022
Published Date: January 10, 2023
Citation: Malik Shahnaz, Snober Malik, Amat us Sami, Sheeba Altafand and Naveed Bashir. (2022) “Profile of Acute Pancreatitis Patients attending a Tertiary Care Teaching Hospital.”, Aditum Journal of Clinical and Biomedical Research, 5(1); DOI: http;//doi.org/07.2022/1.1092.
Copyright: © 2023. Amat us Sami. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
Acute pancreatitis (AP) is a common digestive disease and the most frequent disorder of the pancreas. It is an inflammatory process of the pancreas, with variable involvement of other regional tissues or remote organ systems.
Introduction:
The term pancreas was coined by RUFUS of Ephesus (100 A.D).The name pancreas is derived from the Greek ‘pan’ meaning all and ‘kreas’ meaning flesh.
Anatomy:
The gland weighs approx. 80 grams and is situated retroperitoneally. It is divided into a head, which occupies 30% of the gland by mass, and a body and tail, which together constitute 70% of the whole organ.
Surgical physiology:
In response to a meal, the pancreas secretes digestive enzymes in an alkaline (pH 8.4) bicarbonate rich fluid. Spontaneous secretion is minimal. About 90% of protein synthesized in the pancreas is exported from the acinar cells as a variety of digestive enzymes. These proteins move from
Etiology:
It is important to clarify the underlying cause of an attack of AP because the etiology will affect decision-making and further therapeutic procedures targeted at preventing the development of chronic pancreatitis. Worldwide, gallstones are the most common cause of AP, accounting for approximately 45% of cases, alcohol being the second most common, accounting for 35% of cases. The proportion of the two main causes depends on geographic and cultural factors. In southern Europe, gallstones are the predominant cause of AP, whereas central and northern Europe see a similar frequency of the two factors, or a predominance of alcohol. In studies from the U.K and Asia, gallstone-induced AP predominates, whereas in the U.S.A, alcohol is the main cause. There is a predominance of men in those studies where alcohol is the main etiology of AP, and the mean age tends to be low in this group of patients. Other rarer causes of AP include various drugs, trauma (accidental or iatrogenic), ERCP, metabolic abnormalities (hypertriglyceridemia, hypercalcemia), obstruction (tumors, pancreasdivisum, choledochocele), infections (viral, parasitic, bacterial).
Pathogenesis:
As early as 1896, auto digestion of the pancreas by premature activation of pancreatic proteases was suggested as an essential event in the pathogenesis of acute pancreatitis, resulting in a disease ranging from mild pancreatic interstitial edema to large confluent necrosis of pancreatic and peripancreatic tissue. Considerable interest has focused on the mechanisms by which these enzymes might become activated, prematurely, causing pancreatic injury. The premature activation of trypsinogen to trypsin in the acinar cell in the pancreas is considered a possible key event in the development of acinar cell injury, leading to autodigestion. In most cases, AP is a mild self-limiting disease that resolves spontaneously without complications, but the severe necrotizing form of the disease, which occurs in about 20% of attacks, is a life threatening condition with high morbidity. Mortality may reach 40%, especially if bacterial contamination of the pancreatic necrosis occurs. An improved outcome in the severe form of AP is based on early identification of disease severity and subsequent focused management of these high-risk patients.
Diagnosis:
The diagnosis of AP relies on a combination of clinical evaluation and the use of supportive laboratory and radiological investigations.
A. Clinical assessment:
B. Laboratory diagnostics:
Several other markers have been evaluated as diagnostic tests for AP, including:
-Serum elastase,
-Phospholipase A2,
-Pancreas-specific protein (procarboxylpeptidase B) ,
-Pancreatic isoamylase,
All these appear to offer no advantage over amylase and lipase.
C. Imaging:
Severity assessment of acute pancreatitis:
In the majority of cases, AP is a mild self-limiting disease with a mortality of less than 2%. However, about 20% of all cases develop severe disease, and despite considerable improvements in treatment, mortality remains between 15% and 25%, in severe cases and reaching up to 40% if pancreatic necrosis is infected.
Early prediction of severity is important as within the first 48 hours there is a therapeutic window when specific treatment alternatives may alter a patient’s outcome. Beneficial results have been obtained with the early management of patients, correctly classified as severe, in intensive care units, with early ERCP in gallstone-induced disease, and prophylactic antibiotics. Conversely, reliable exclusion of patients with severe AP helps to avoid unnecessary use of invasive and otherwise costly procedures in mild cases, thereby facilitating optimal use of limited health care resources.
Objective:
Profile of Acute Pancreatitis Patients attending a Tertiary Care Teaching Hospital
Material and methods:
The present study was conducted for the period from Nov 2010 to Oct 2011 in the Acharya Shri Chander College of Medical Sciences and Hospital, Sidhra, Jammu. Patients admitted in the surgery and allied departments of this hospital were enrolled in the study after fulfilling the eligibility criteria including a written informed consent after explaining the study to the patient
Results:
A total of 100 cases were studied.
Age distribution:
All the patients of acute pancreatitis who presented to hospital till the sample size was fulfilled were included irrespective of age. The youngest patient in our study was a 14 year old who was admitted as a case of traumatic pancreatitis and the oldest patient was a 72 year old female patient. Maximum number of patients was in the age group of 41-50 years.
|
Age group |
No of patients |
|
0-10 |
0 |
|
11-20 |
4 |
|
21-30 |
11 |
|
31-40 |
15 |
|
41-50 |
47 |
|
51-60 |
18 |
|
61-70 |
4 |
|
71-80 |
1 |
|
Total |
100 |
Table1: Age distribution
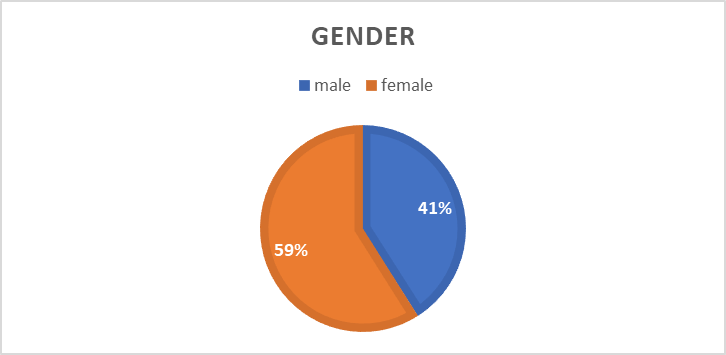
Sex Distribution:
The cases were included in the study irrespective of their individual sex. However the following observation was made as regards the sex distribution of the cases.
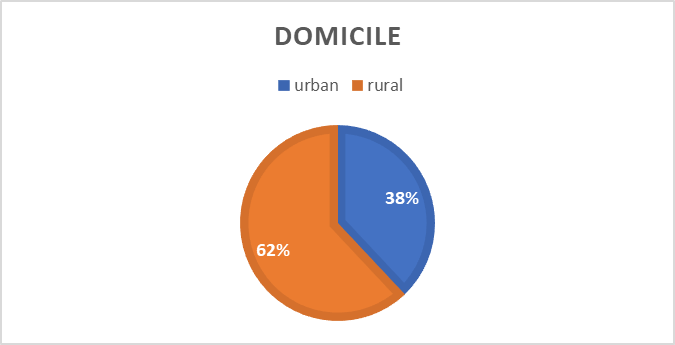
Geographical distribution:
It was seen, that there was a marginally higher number of rural patients in our study, probably reflecting the pattern of admissions in our hospital in general.
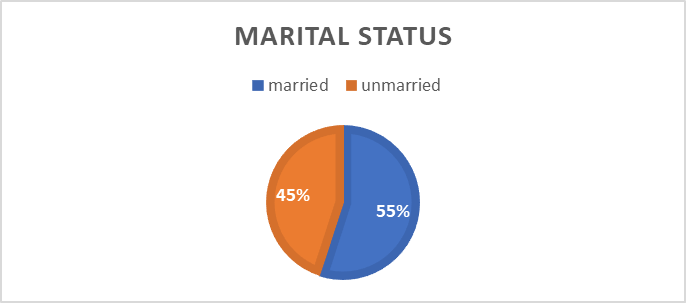
Marital status:
|
Etiology:
|
Discussion:
Acute pancreatitis is a common ailment encountered by the surgeons, in any part of the world, and forms a good proportion of emergency admissions in surgical emergency units. Even though the diagnosis of pancreatitis has become easier by the measurement of specific pancreatic enzymes there are still 30%– 40% of the fatal cases which are first diagnosed at autopsy. It is of utmost importance to assess the diagnosis and the severity of acute pancreatitis in the beginning to identify those patients with severe or necrotizing disease who benefit from an early initiated intensive care therapy. Additionally, in view of new therapeutical concepts (e.g. antibiotic therapy in severe forms) and for the evaluation of new drugs, patients should be staged into mild and severe disease as early as possible. In most cases it is not possible to assess the severity clinically on hospital admission. This study was conducted to evaluate the sensitivity and specificity of C-reactive protein(CRP) and APACHE II in determining the severity of Acute pancreatitis so that early intensive therapy can be initiated.
In our study, as far as the sex ratio is concerned, females outnumbered males and the male to female ratio was 1: 1.43.
Antonio carnovale’s study of 1,135 patients had a male to female ratio of 1: 1.6 (431 males and 704 females).
W Uhl study of 302 patients has a male female ratio of 1.85: 1.
Study of Minguez M had a male to female ratio of 1: 1.4.
T K Choi repoted a male to female ratio of 1: 1.1.
A C de Beaux study had a male to female ratio of 1.6: 1.
The female preponderance in our study conflicts with most other studies done world over. The possible explanation is the fact that alcoholism which forms a major cause of pancreatitis in the western world, is found much less often as a cause of pancreatitis in this part of the world, because of a conservative society pattern.
The commonest etiological factor in our study was biliary tract pathology which included gallstones (47%) and alcohol abuse (26%)
W Uhl etal, in their study had a biliary tract pathology in the range of 36-38%.
Marshall J B, found Biliary pathology and alcoholic abuse as a cause of acute pancreatitis in 60-80% of patients.
Minguez, found biliary pathology causative in 52% of patients of acute pancreatitis.
Steinberg etal mentioned that biliary disease is the most common cause of AP in the United States, Asia and most of Western Europe (1994).
A Biliary cause of pancreatitis was noted in a higher percentage of patients in our study; Moreover, Alcoholism which forms a major etiology in the western world is not as prevalent in this part of the world.
Presenting symptoms in our study were, abdominal pain
(100%) followed by nausea and vomiting (80%), distension
(19%), fever (6%), constipation (2%) and breathlessness
(4%).
Webster P D reported nausea and vomiting in 75-90% of patients.
The abdominal findings on presentation in our patients were tender epigastrium in 88% patients, guarding (35%). None of our patients had bleeding into fascial planes on presentation.
Webster P D reported abdominal pain and guarding in 50-90% of patients.
Sheehy reported a similar incidence in his study.
32 patients (32%), in our study developed severe pancreatitis according to Atlanta classification. Similar results were seen in other studies.
Marko Lempinen et al noted development of severe pancreatitis in 28% of their cases.
M Winslet etal noted severe pancreatitis in 27% of admitted patients.
Overall mortality in our series was 3%, all the three patients belonged to the severe acute pancreatitis group. Similar results were seen in other studies world over.
Steinberg W noted a mortality of 2-9% in his study.
Minguez W reported a mortality of 5.1% in his study.
Luengo reported a mortality of 2% in controls.
Mann et al. , Banerjee et al. , and Grönroos et al. separately noted that in acute pancreatitis the average mortality rate approaches 2-10% .
Majority of patients in our study were in the age group of 41-60 yrs. The age range was 11-80yrs.
Antonio Carnovale, in his study had an age range of 18-93yrs with a median age of 61.5 yrs.
In the study by W Uhl the mean age was 50yrs.
The age range in the study by A C de Beaux was 11-93yrs with a median age of 53yrs.
The mean age was 42.9±15.9 years (range: 18-80 years) in the study by Raghu M G etal.
A median age of 45 years (range, 20–94), was seen in study by Marko Lempinen et al.





Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org