Aditum Journal of Clinical and Biomedical Research
OPEN ACCESS | Volume 8 - Issue 1 - 2026
ISSN No: 2993-9968 | Journal DOI: 10.61148/2993-9968/AJCBR


Wijegunasekara J.L.H.R *1, Jayalal T. B. A. 2, Rathnayaka R. M. S. S 3
*1Deputy Director, De Soyza Hospital for Women (Teaching), Colombo, Sri Lanka.
2Deputy Director General (Dental Services), Ministry of Health, Sri Lanka
3Senior Registrar (Medical Administration) Ministry of Health, Sri Lanka.
*Corresponding Author: Wijegunasekara J.L.H.R, Deputy Director, De Soyza Hospital for Women (Teaching), Colombo, Sri Lanka.
Received: April 28, 2021
Accepted: May 03, 2021
Published: May 10, 2021
Citation: Wijegunasekara, Jayalal and Rathnayaka. (2021) “Compliance with Covid - 19 workplace safety guideline: by employees at “Suwasiripaya”, Colombo”, Aditum Journal of Clinical and Biomedical Research, 2(2); DOI: http;//doi.org/04.2021/1.1031.
Copyright: © 2021 Wijegunasekara. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background:Adherence to workplace safety guideline with regard to Covid -19 is a responsibility of employees working in every workplace. “Suwasiripaya”, the head - quarters of the Ministry of Health is a highly congested workplace with a suspected gap in the adherence of the employees to this guideline.
Objective: This study was carried out to assess the compliance of employees at “Suwasiripaya”, Colombo, to Covid – 19 workplace safety guidelines of Environment and Occupational Health directorate of Ministry of Health and to identify any gaps to recommend corrective measures.
Methods: It is a descriptive cross-sectional study carried out in “Suwasiripaya”. Convenient sample of 10% of the total population of 1350 employees were selected and quota sampling method was used to divide the sample among 08 staff categories. Data was collected in a single day survey using a Self – Administered Questionnaire, prepared in consistent with covid - 19 workplace safety guideline. Compliance was assessed using direct responses and responses of 4-point Likert scales. Quantitative analysis was carried out for closed ended questions and the open-ended question was thematically analyzed.
Results: Response rate was 96.3%. 53.8% of the staff were development officers and management assistants. 76.2% says that their risk assessment was not done by the unit. 33.8 % says that covid workplace guideline was not formally delivered to them. 53.8% had an awareness about the guideline only to some extent.
The compliance of the employees with administrative requirements, personal hygienic measures, cleaning measures and overall compliance were 50.50%, 49.23%, 23.60% and 41.11% respectively. Open ended question has provided with recommendations from employees’ perspective, under 08 themes.
Conclusions: Employee compliance with the guideline is poor. Employees’ suggestions; staff education; to limit staff; to improve personal protective measures; to improve supervision; law enforcement; to improve resources and other managerial changes are recommended to improve the compliance.
Introduction:
Novel beta - corona virus (2019 - n CoV) or Covid - 19 is the pandemic out - break of Severe Acute Respiratory Syndrome Coronavirus - 2 (SARS - CoV - 2) respiratory illness [1] which has infected 19.5 million people and caused 675,000 deaths in more than 200 countries all over the world since 31st of December 2019 up to 10 of August 2020 [2] and still continue to spread further, resulting in a devastating public and occupational health crisis [3].
World Health Organization (WHO) and many other relevant authorities are providing with necessary technical guidance in the form of guidelines, protocols, policies and procedures to instruct the countries and the people for the control of disease transmission, patient load and the number of deaths. This technical guidance provides with accurate information to obtain the required knowledge to be translated to essential practice [3, 4, 5,6,7,8,9].
Worldwide, all the countries are practicing these guidelines, developed internationally and nationally according to the need of the country. However, there are possible gaps in the implementation process in almost every country explaining the existing failure to control the disease as expected [2].
Sri Lanka too has been combating with the disease for the last four months using numerous infectious disease control measures and evidence based strategies; namely personal and environment hygienic practices and social distancing to control the transmission (10).As a result, country has been able to contain the disease at stage - 3 level of disease transmission; i.e. “limited to community clusters” with no large out breaks of community transmission [5].
Now, the country is gradually entering to an era of “ new normal” [11]where country has restarted its lost economic activities in both public sector and private sector while carrying on the new way of behavior strictly adhering to guidelines for work place safety for various sectors in the country issued by the Ministry of Health [12]. Hence, Employees’ compliance to guidelines is essential to safeguard the country from the risk of the second wave of the disease as seen in some other well performed countries.
“Suwasiripaya” is the busy head - quarters of Ministry of Health and the focal point of the public health system in Sri Lanka. It lies in a highly populated location in the capital city, Colombo and more than 1000 staff members are employed in a very constrained infrastructure.
With respect to Covid - 19 transmission, it is also another workplace requiring good compliance among employees with workplace safety guidelines. The image of behaving as a role model also needs to be safe guarded. To date it is not clear if employees’ practices are in line with the recommended guidelines for workplace safety.
As the leading workplace in the endeavor of battling against the corona pandemic, it is essential to know about its own compliance with the expected practices, to identify gaps if any and to recommend corrective measures to upgrade the situation.
Therefore, this research study was conducted to assess the compliance of employees working in “Suwasiripaya” to the occupational safety guidelines of Environment and Occupational Health (E & OH) directorate of Ministry of Health. The results of the study will enable to map a way forward so as to improve worker practices to improve workplace safety.
Objective:
This study was carried out to assess the compliance of employees at “Suwasiripaya”, Colombo, to Covid – 19 workplace safety guidelines of Environment and Occupational Health directorate of Ministry of Health and to identify any gaps to recommend corrective measures to improve adherence.
Specific Objectives:
Methods:
Study design:
It is a descriptive cross-sectional study.
Study setting:
It was conducted in “Suwasiripaya” i.e. headquarters of Ministry of Health, Sri Lanka.
The total population of 1350 staff members permanently employed in all the units can be categorized basically into eight categories namely, administrative staff (60), accountants (10), medical officers (48), development officers (277), public/health management assistants (348), karyala karya sahayaka (55), saukya karya sahayaka (362) and drivers (191).
Sampling:
The total population of 1350 staff members who are currently working at the premises of “Suwasiripaya” was taken as the study population. Employees in active operation on the day of the survey were included and those who were on “work from home” were excluded. However, exclusion of this group is not expected to introduce any bias to the study because units have made them “work from home” on a roster basis where every staff member had an equal chance to “work from home”.
10 % of the total population was taken as a convenient sample size because the quick findings were very valuable to identify any gaps to take corrective measures without delay.
Calculated sample size (N = 135) was divided among staff categories, in proportion to the number of staff working in each category using quota sampling technique.
Data collection:
Data was collected using a Self – Administered Questionnaire which was prepared in line with the E & OH safety guideline. It consisted of 44 closed ended questions on demographic variables; employee’s high risk factors; employee’s awareness on the guideline; compliance with the managerial measures, personal safety measures and housekeeping measures stated in the guideline and an open ended question to receive their suggestions for improvement.
Compliance was defined as practice of the E&OH safety guideline.
This single day survey was conducted by the study team, with the participation of predetermined number of employees from each staff category. Care was taken to involve almost all the units in “Suwasiripaya.” Data was collected from consented participants. Data was checked for completeness and accuracy. Confidentiality and data security were maintained.
Analysis:
Data was analyzed using IBM SPSS Statistics (version 21) to obtain descriptive frequencies and proportions of employees who comply with each statement of the guideline. Answers for open ended questions were thematically analyzed.
Results:
1. Results of closed ended questions:
Response rate was 96.3%. 53.8% of employees were development officers and management assistants. Highest number of 40% were in the age group 31 - 40 years. 60% were females. 41.5% were degree holders. 63.1% had a service period of < 10 years. Only 3.1% and 2.3% were suffering from high risk diabetes and heart diseases. (Table 1)
|
No |
Variable
|
Frequency |
Percentage % |
|
1 |
Staff category |
||
|
|
Manager |
6 |
4.6 |
|
|
Medical Officer |
6 |
4.6 |
|
|
Develoment Officer/ Management Assistant |
70 |
53.8 |
|
|
Karyala Karya Sahayaka |
10 |
7.7 |
|
|
Saukya Karya Sahayaka |
19 |
14.6 |
|
|
Driver |
19 |
14.6 |
|
|
Total |
130 |
100 |
|
|
|
|
|
|
2 |
Age category |
||
|
|
20-30 |
32 |
24.6 |
|
|
31-40 |
52 |
40 |
|
|
41-50 |
38 |
29.2 |
|
|
51-60 |
6 |
4.6 |
|
|
>60 |
2 |
1.5 |
|
|
Total |
130 |
100 |
|
|
|
|
|
|
3 |
Gender |
||
|
|
Female |
78 |
60 |
|
|
Male |
52 |
40 |
|
|
|
130 |
100 |
|
|
|
|
|
|
4 |
Education level |
||
|
|
Ordinary level |
22 |
16.9 |
|
|
Advanced level |
54 |
41.5 |
|
|
Degree holder |
54 |
41.5 |
|
|
Total |
130 |
100 |
|
|
|
|
|
|
5 |
Period of service (years) |
||
|
|
<10 |
82 |
63.1 |
|
|
11 -20 |
31 |
23.8 |
|
|
21 -30 |
16 |
12.3 |
|
|
>30 |
1 |
0.8 |
|
|
Total |
130 |
100 |
|
|
|
|
|
|
6 |
Suffering from high risk conditions? |
||
|
|
Diabetes |
4 |
3.1 |
|
|
Heart diseases |
3 |
2.3 |
|
|
Respiratory diseases |
1 |
0.8 |
|
|
Other immune deficiency diseases |
1 |
0.8 |
|
|
Not belong to any |
121 |
93.1 |
|
|
Total |
130 |
100 |
Table 1: Frequency distribution of demographic factors of employees.
76.2% said that their risk assessment with regard to covid 19 was not done by the unit. 33.8 % said that covid work place guideline was not formally delivered to them. 53.8% had an awareness about the guideline only “to some extent”. 59.2% has received this information from self - reading. Only 10.8% had received the information from supervisors. 21.5% said their knowledge on the guideline is “very adequate” and 44.6% said their knowledge on the guideline is “adequate”. However, 20.8% said their knowledge was “moderately adequate” and 13.1% said it was “not adequate”. (Table 2)
|
No |
Variable
|
Frequency |
Percentage % |
|
1 |
Whether risk assessments done? |
|
|
|
|
Yes |
8 |
6.2 |
|
|
No |
99 |
76.2 |
|
|
Not relevant |
23 |
17.3 |
|
|
|
130 |
100 |
|
8 |
Whether information regarding the guidelines was delivered formally? |
||
|
|
Yes |
82 |
65.1 |
|
|
No |
44 |
33.8 |
|
|
Not relevant |
4 |
3.1 |
|
|
Total |
130 |
100 |
|
|
|
|
|
|
9 |
Awareness of the guideline? |
||
|
|
Very clear |
51 |
39.2 |
|
|
Some extent |
70 |
53.8 |
|
|
None |
9 |
6.9 |
|
|
Total |
130 |
100 |
|
|
|
|
|
|
10 |
Ways of receiving information? |
||
|
|
Self-reading |
77 |
59.2 |
|
|
From peers |
14 |
10.8 |
|
|
From supervisors |
14 |
10.8 |
|
|
From head of institution |
8 |
6.2 |
|
|
Special meeting |
3 |
2.3 |
|
|
From many ways |
14 |
10.8 |
|
|
Total |
130 |
100 |
|
|
|
|
|
|
11 |
Adequacy of knowledge on the guideline? |
||
|
|
Very much adequate |
28 |
21.5 |
|
|
Adequate |
58 |
44.6 |
|
|
Moderately adequate |
27 |
20.8 |
|
|
Not adequate |
17 |
13.1 |
|
|
Total |
130 |
100 |
|
|
|
|
|
Table 2: Frequency distribution of employee responses regarding the covid 19 – workplace safety guideline.
With regard to administrative requirements, 76.9% compliance was seen with “daily temperature checking”. “Availability of attendance schedule”; “attention on high risk when scheduling duties”; and “appointing a special officer in units for supervision of covid preventive measures”; had only 52.3%, 43% and 30% compliance respectively. (Figure 1)
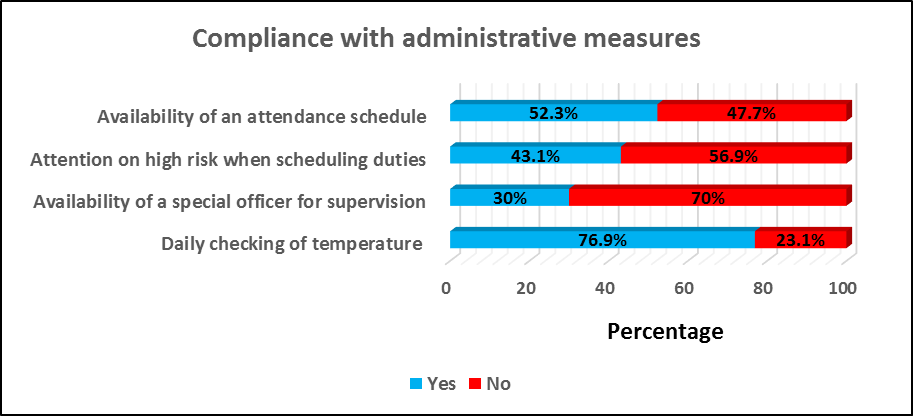
Figure 1: Compliance of the employees with the administrative measures in the guideline.
With regard to personal hygienic measures described in the guideline, nearly 90% were compliant with “staying at home when they had respiratory symptoms”; “washing their hands at the entrance to the work place”; “ implementing recommended practices when entering and inside the home”. However, only 26% were compliant with “different time intervals allocated for lunch”. (Figure 2)
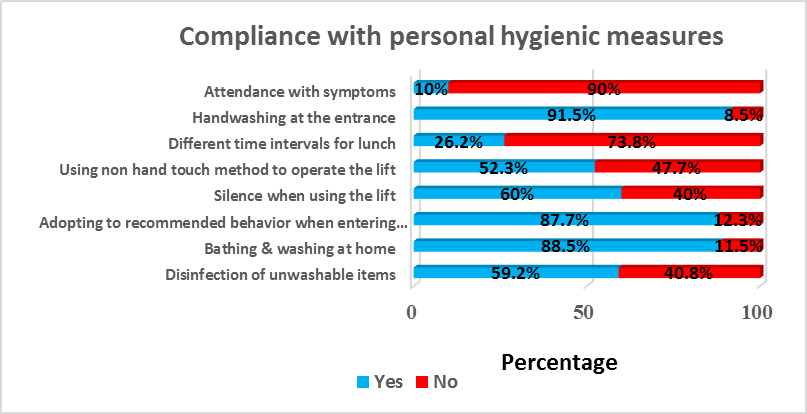
Figure 2: Compliance of the employees with the personal hygienic measures (first set) in the guideline
73%, 66%, 62%, 62% and 55% were compliant with “using a face mask while working”; “not using common utensils”; “disposal of masks into a closed bin”; “bringing food from home”; “chatting with peers”; and “carefulness of using currency” respectively. However, only 40%, 35.4%, 27% and 20% compliance were seen with “hand washing after touching documents”, “hand washing after touching objects”, “social distancing” and “controlling outsiders visiting the place”. (Figure 3)

Figure 3: Compliance of the employees with the personal hygienic measures (second set) in the guideline.
With regard to the house keeping measures described in the guideline; only 30% compliance was seen with “washing office floors and office instruments at expected frequency”. Only 28.5% compliance was seen with “maintaining proper ventilation”. Further, 55.4% were never reported to “washing door knobs and handles in the office room”. (Figure 4)

Figure 4: Compliance of the employees with the cleaning measures in the guideline.
In summary, compliance of employees to cleaning measures, personal hygienic measures and administrative requirements are 23.60%, 49.23% and 50.50% respectively. Overall compliance of employees to the work place safety guideline is 41.11%. (Figure 5)
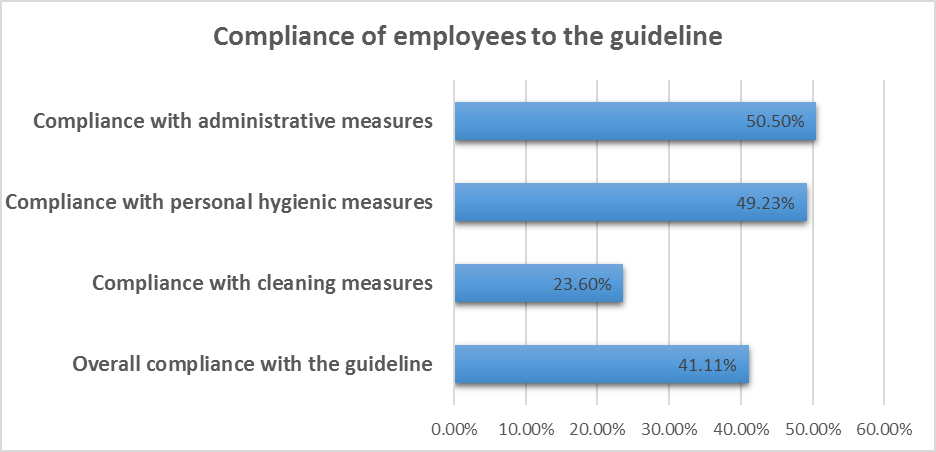
Figure 5: Percentage distribution of overall compliance of employees with the guideline.
(2). Results of the open-ended question:
Suggestions to improve employee adherence to workplace safety guideline according to perception of employees were collected in the open ended question. Response rate was 71.8%. The responses were categorized into 08 themes. The number and the percentage of respondents who have given different responses under each theme were calculated and summarized. (Table 3).
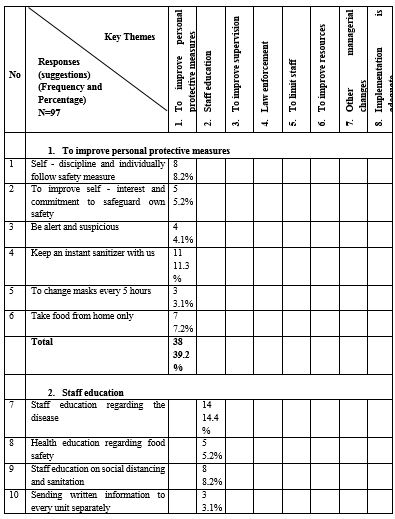
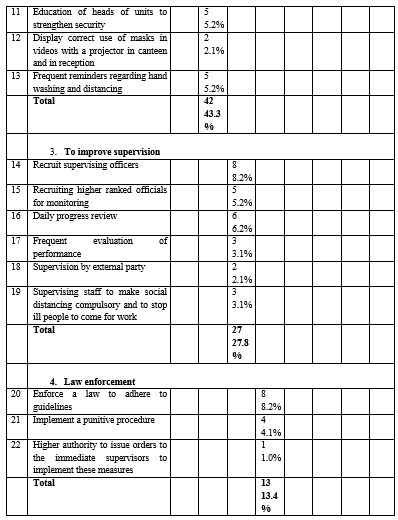
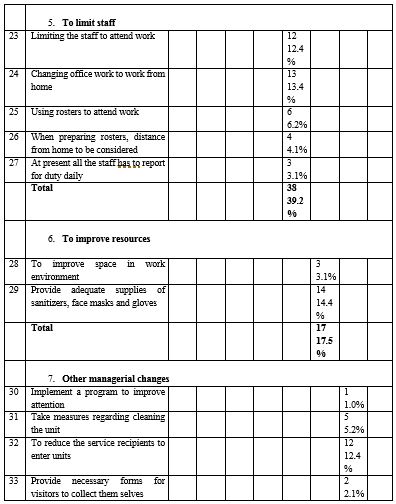
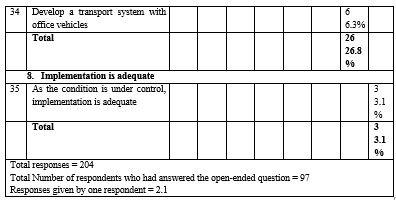
Table 3: Distribution of employee responses (suggestions) to improve adherence to workplace safety guideline under 08 key themes.
Different suggestions from employees to improve adherence to workplace guidelines, categorized into 08 key themes are as follows; 1. Staff education (43.3%) 2. To improve personal measures (39.2%) 3. To limit staff (39.2%) 4. To improve supervision (27.8%) 5. To improve resources (17.5%) 6. Law enforcement (13.4%) 7. Other managerial measures (26.8%) and 8. Agreed as implementation is adequate (3.1%). (Figure 6)
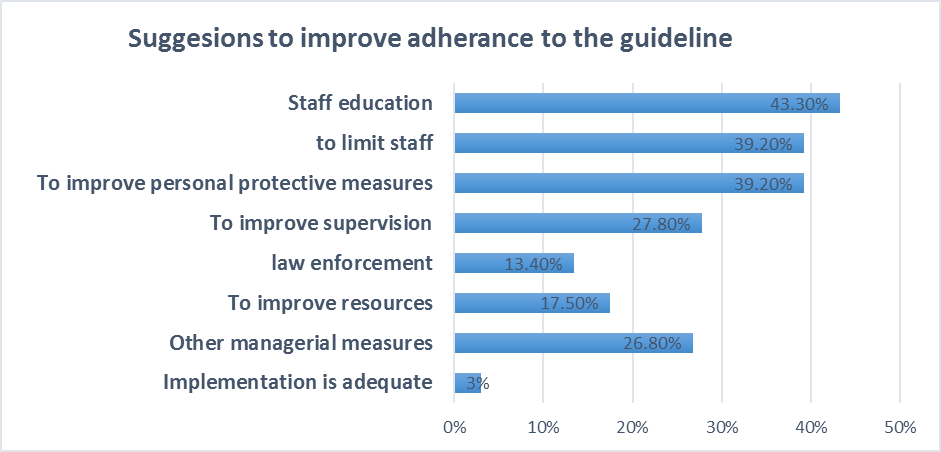
Figure 6: Percentage distribution of key themes of employees’ suggestions, to improve employee adherence to workplace safety guideline.
Some of the very important individual suggestions which were selected from 08 themes are as follows; 1. Employees to be self - disciplined and individually to follow safety measures, 2. To keep an instant sanitizer with the employee, 3. To take food from home, 4. Staff education regarding the disease, 5. To recruit supervising officers, 6. To perform daily progress reviews, 7. To enforce a law to adhere to guidelines, 8. To change “office work” to “work from home”, 9. To consider the distance to home when preparing rosters, 10. To provide adequate supplies of sanitizers, face masks and gloves, 11. To reduce the number of service recipients entering the unit, 12. To strengthen measures in cleaning the unit and 13. To develop a transport system with office vehicles. (Figure 5)
3.1% said that “as the condition is under control, implementation is adequate”. (Figure 5)
Discussion:
Compliance to guidelines in response to covid - 19 pandemic reduces the likelihood of both contracting the virus and infecting others (1, 2, 4). To implement full compliance to guidelines is doubtful in a democratic society. However, it is in managers’ hands to maximize the implementation process of guidelines (6).
Managers should be well aware of the technical facts explained in the guideline, should make the responsible people educated, provide adequate resources for implementation, motivate the relevant people to comply with the guideline, frequently reminding and monitoring their compliance and take corrective actions where the compliance seems to be poor (13).
This study showed that compliance of the employees with administrative measures, personal hygienic measures and house - keeping measures is; 50.5%, 49.23%, 23.6% respectively. Overall compliance to the workplace safety guideline is 41.11%. Compliance of employees to selected measures were “good” as in staying at home when having symptoms (90%), daily checking temperature (76.9%), washing hands at the entrance (91.5%), using masks during working (78.5%), bringing food from home (61.5%) and precautions when entering home (87.7%). This high level of compliance seems to be with decisions taken at higher managerial levels. This indirectly shows that management concern could highly influence the employees’ compliance with this guideline.
However, compliance was “moderate” or “poor” with most of the other measures. Majority of them are activities happening repeatedly such as hand washing after touching documents and objects, sharing objects, frequent washing floors, surfaces and instruments, social distancing etc. Hence, strengthening personal protective measures, staff education, strengthening supervision, law enforcement, preparation of suitable duty rosters, strengthening crowd control measures, had been identified by the employees to improve compliance with this guideline. Education, knowledge, favorable attitudes, financial constraints and subjective norms are some general causes identified in other studies. [15]
Further, 53.8% had an awareness about the guideline only to some extent. This guideline seems to be not well communicated with the employees. Communication could have been further limited by poor literacy of English language among employees. Therefore, all efforts need to be made to translate guidelines to Sinhala and to educate them in their native language. In addition, this guideline could have been prepared at several levels targeting at different categories at different levels of understanding.
In particular, Guidelines should be considered as very important documents to guide people in the expected direction. Attention should be paid on each and every instruction given, especially in infection control measures (15) because one instruction not followed could act as the sole source of disease transmission. Further, if guidelines for work place safety are not fully practiced, there is a very high chance of breaching social distancing in this congested study setting which can lead to easy person to person transmission of the disease and creation of a cluster even if a single person happens to contract the disease.
In conclusion, the adherence of the employees to the workplace safety guideline was found to be sub optimal which needs urgent correction. Answering to this questionnaire itself seems to be an eye opener to the employees to identify the areas they should focus more at this critical period. Further, it is brought to the attention of the higher management in “Suwasiripaya”, the suggestions provided by the employees from their own perspective, to be implemented as recommendations to improve safety in this work setting.
Limitations:
Assessment was based on respondents’ own determination and admission rather than independent observation of their actual practice. However, emphasis on the value of their inputs for improvement initiatives and their anonymity should have improved the actual reporting. In contrast, a considerably high percentage of respondents admitting poor compliance with many measures in the guidelines too indicates that the results obtained seem to represent the real picture.





Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org