
Jessy Mavarayil John1*, Riju Sharma2
1Research Scholar, Department of Social Work, Assam Don Bosco University, Guwahati, India.
2Research Guide & Director School of Social Sciences, Assam Don Bosco University, India
*Corresponding author: Jessy Mavarayil John, Research Scholar, Department of Social Work, Assam Don Bosco University, Guwahati, India.
Received: March 06, 2021
Accepted: March 15, 2021
Published: March 30, 2021
Citation: J Mavarayil John, R Sharma “Effectiveness of life skill training to enhance mental health and wellbeing of young people: does peer group involvement matter?”, 2(2); DOI: http;//doi.org/03.2021/1.1012.
Copyright: © 2021 Jessy Mavarayil John. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly Cited.
Aim of this study is to assess the effectiveness of life skills training and the influence of peer groups on mental health and wellbeing of young people. A classical experimental research design with control group and random sampling method was used. This study comprises 720 young people (both girls and boys in the age group of 16 to 19yrs) from six higher secondary schools of Kerala. The respondents were sequentially assigned into intervention group and control group with 360 students each for determining the effect of intervention comparatively. The data collection was done in three time lines: pre-intervention, post-intervention and follow-up intervention. Standard tools used to evaluate mental health and wellbeing was: GHQ-28 (Goldberg, 1997) and WEMWS-14 (Warwick Edinburg Mental Wellbeing Scale, 2007) respectively. Researcher conducted life skills training to the intervention group after pre - intervention. The same assessment tools were administered post- intervention and follow - up intervention to evaluate the effectiveness of LST. Repeated Measures Analysis of Variance (RMANOVA) was performed to test whether there is any significant effect due to intervention in the scores. Independent sample t-test was performed to compare the equality of baseline scores of various components.
The result showed that there was highly significant intervention effect between the scores of mental health and wellbeing due to life skill training. And also, it is clear that the involvement in peer group is significant in post- intervention scores in various components of the intervention group. It is observed that somewhat / balanced involvement is better for maintaining good mental health status and wellbeing among young people.
Introduction And Review Of Literature
Mental health is fundamental to good health and quality of life and globally, there has been an increasing recognition of the importance of mental health and wellbeing to overall health (WHO, 2004 & Mental Health Foundation; NIMHE, 2005). Mental health status of an individual encompasses both cognitive and emotional resources, which gets enhanced or depleted throughout the life course. Mental wellbeing is referred to as an individual’s ability to develop their potential, work productively and creatively, build strong and positive relationship with others and contribute to their community (Beddington et al., 2008).
Studies say that mental health status of adolescents can affect their overall wellbeing in both immediate and longer-term goals. WHO says, worldwide up to 20% of adolescents suffer from disabling mental health problems. Furthermore, there are close links between child and adult mental illness – the presence of mental illness during childhood may lead up to 10 times higher costs during adulthood (WHO, 1994 & 2001; Suhrcke et al., 2007).
Young age is critical for laying the foundations for good mental health and wellbeing which in turn affect their path through life and healthy functioning of families and society as a whole. Poor mental health in childhood is associated with increased risk in life and other adverse outcomes in adulthood. Schools, communities and families can make the most of its environment favourable to foster mental health and wellbeing of children and adolescents (Kessler et al., 2005: Kieling C. et al., 2011: Murray, et al., 2008).
Young people are one of the precious resources in every country and play a major role in shaping the future of the nation. It is a period characterized by a time of indecision, despair, and doubt, especially in instances where they are not mentally conditioned and physically prepared to cope with the changes taking place in and around them. It is a delightful period of life and a period marked by stress and conflict in the family also. According to Erickson, Adolescents are caught up in an identity crisis, one which is not easy to define; they cannot wait, because it is a period which is fleeting (Erickson, 1968).
There are many strategies to improve mental capabilities, some may want to learn and be enlightened about new things; others can be socially active through engaging religious activities or physical activities like sports / games etc. The available literature indicates that life skills training is needed for young people and should be developed in all culture. Evidences suggest that life skills approach promotes social, cognitive, emotional, behavioural and psychological competencies among young people. Early intervention and life skills training would be beneficial for reducing crime and levels of risk factors. It improves productivity, academic performance, motivation, and numerous positive attitudes, social adjustments, healthy life styles, and foster discipline to enhance self awareness and self esteem that reduces high risk behaviour and increase coping skills and resilience to stress and preserve mental health and wellbeing in older age too (Belay Tefera Kibret, 2016 ; Cooper et al., 2009 ; Bhave Swati, 2005).
Teaching life skills and the involvement in peer groups help young people competent to face the realities of life in order to achieve mental health and wellbeing in certain extend. There is good evidence that mental health promotion programs in schools lead to positive mental health, social and educational outcomes among the students (Weare K., Nind M., 2011).
World Health Organization has addressed life skill based education since the 90s, across culture, life skills training is similar in three important ways such as: a) learning of life skills essentially helps to promote mental health and well being and enables one to deal with everyday challenges, b) life skills education enables adolescents to learn and practice skills, as it is based on student centred and activity oriented methodology, and c) life skills education is based on the philosophy that young people should be empowered to take more responsibility for their actions (WHO 1993a, 1994, 1996, 1997; Bhave Swati, 2005; Vranda, 2015; Guardian & MINDS found,2017; WFMH-Report, 2018).
Some studies say that peer group can be an effective and significant influence for good mental health. Healthy friendship is a crucial element in protecting our mental health and wellbeing. Studies say that healthy friendships can play a key role in helping people to lead a healthy and happy life and overcome the isolation that often comes with it. Healthy friendship is effective to maintain psychological wellbeing and it lead to balance one’s mental health status. People with more severe forms of mental illness have smaller social networks than others and have more family members than friends in their social circle (Mental health foundation, 2019). In line with the previous studies, the researcher trying to assess the effectiveness of Life Skill Training and the Influence of Peer group involvement on Mental Health and Wellbeing of young people. The research methodology and the result and findings are given bellow.
Research Methodology
This study was done with the objectives: (a) to study the effectiveness of life skill training on mental health and wellbeing, and (b) to study the influence of peer group involvement on mental health and well being of young people.
Population And Sample
This study was done on a sample of regular school going higher secondary students in Kerala, (between 16 to 19 years of age group), excluding those with any physical or mental illness and those who have had any life skill training. We selected a control group of 360 students and an intervention group of another 360 students, both with equal proportion of boys and girls. Proportionate random sampling was adopted to select the subjects from schools which are different by their offer of co- education or exclusive (gender selective) admission policy. All of them were subjected to mental health and wellbeing assessment at the pre-intervention phase. The intervention group was given life skill training and they were assessed in two follow up periods after three months and six months. The control group was also assessed simultaneously, but they were given life skill training in view of our moral commitment to them, shortly after their final assessment.
Data Collection Method
For this study primary data has been collected and it obtained from July 2017 to January 2019 in three different timelines of pre, post and follow-up intervention.
Tools Used For Data Collection
The following tools were used for data collection in three timelines are: Demographic proforma and Standardized tools of General Health Questionnaire (GHQ-28) and Warwick Edinburg Mental Wellbeing Scale (WEMWS-14).
Ethical And Legal Sanctions
This study was approved by the University Ethics Committee of Assam Don Bosco University. Permission granted from the Regional Deputy Director (Dept. of Higher Secondary Education) and the principals of the concerned schools for conducting the study among the students. Informed written consent was obtained from the participants and their parents prior to the study.
Results And Findings
The statistical analysis is based on the objectives of the study are given below:
Repeated measure analysis of variance – RMANOVA- was performed to see the difference between the scores of mental health status and wellbeing of young people due to intervention. The following tables and figures have given the result and findings in three time lines of pre- intervention, post-intervention and follow-up intervention
|
Group |
Mean (Standard Deviation) |
F statistic and p value |
||||
|
Baseline
/Pre-int. |
Post- intervention |
Follow-up intervention |
Time |
Group |
Time*group interaction |
|
|
Control |
29.131 |
28.803 |
28.664 |
F=1438.067 |
F=56.891 |
F=1358.828 |
|
|
(10.752) |
|
|
|
|
|
|
|
|
(10.461) |
(10.298) |
Df=(2, |
DF=(1, |
|
|
|
|
|
|
1436) |
718) |
|
|
|
|
|
|
|
|
DF=(2,1436) |
|
|
|
|
|
P=0.000 |
P=0.000 |
|
|
|
|
|
|
|
|
P=0.000 |
|
Intervention |
30.178 |
13.739(9.126) |
25.294 |
|||
|
|
(11.739) |
|
(11.052) |
|
|
|
Table1 Results of RMANOVA for mental health status scores
The above table describes the extent of change in the mental health status scores among the respondents across the time period of pre- intervention (baseline), post-intervention and follow-up intervention, between the intervention group and control group. There is significant difference in the overall mean score of mental health status between the two groups due to intervention. Since p-value ( p=0.000) is less than 0.05 (normal value) indicating that the intervention is effective.
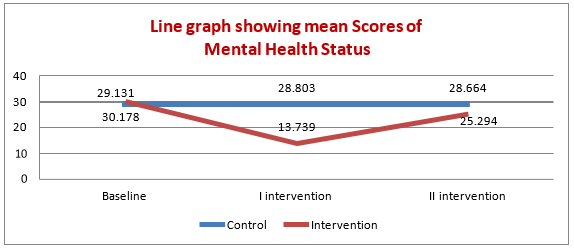
Figure 1 Line graph of the Mean Scores of Mental Health Status
The above line graph shows that, the differences in the average scores are more for intervention group whereas for control group they are not, indicates that intervention is effective.
|
Group |
Mean (Standard Deviation) |
F statistic and p value |
||||
|
Baseline
/Pre-int. |
Post- intervention |
Follow-up intervention |
Time |
Group |
Time*group interaction |
|
|
Control |
43.269 |
43.533 |
43.633 |
F=1435.309 |
F=90.403 |
F=1354.173 |
|
|
(7.453) |
|
|
|
|
|
|
|
|
(7.128) |
(6.927) |
Df=(2, |
DF=(1, |
|
|
|
|
|
|
1436) |
718) |
|
|
|
|
|
|
|
|
DF=(2,1436) |
|
|
|
|
|
P=0.000 |
P=0.000 |
|
|
Intervention |
43.903 |
55.067 |
46.300 |
|
|
|
|
|
(7.975) |
(5.990) |
(7.503) |
|
|
|
Table 2 Results of RMANOVA for mental wellbeing scores
Table 2 describes the extent of changes in the mental wellbeing scores among the respondents across three time lines between intervention group and control group. The result tabulated shows that there is highly significant intervention effect between the scores of mental wellbeing over different time periods and between the two groups. Since p values is less than 0.05 showing that the intervention is effective.
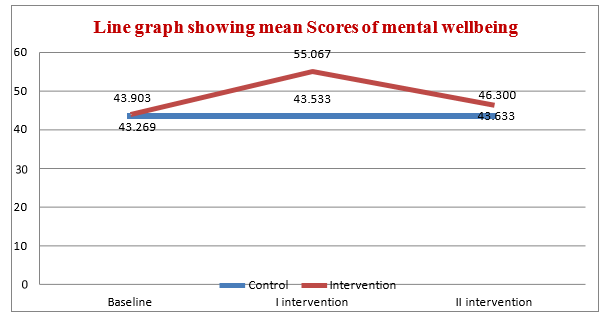
Figure 2 Line graphs of mean scores of mental wellbeing
The above line chart shows that, the differences in the average scores are more for intervention group whereas for control group they are not.
The questionnaire carries question regarding the involvement of peer group. Researcher wanted to see whether there is any significant difference in the scores for those who have involvement with peer group i.e. whether the involvement in peer group helps them to have better mental health and wellbeing. Independent samples t -test was performed to see the difference between the scores of those with and without peer group involvement on various timelines. The results are described in detail in the following section, using the tables as follows
|
Involvement in peer group |
Control Group |
Intervention Group |
||
|
Frequency |
Percent |
Frequency |
Percent |
|
|
Highly involved |
211 |
58.6% |
211 |
58.6% |
|
Somewhat involved |
146 |
40.6% |
145 |
40.3% |
|
Not involved |
3 |
0.8% |
4 |
1.1% |
|
Total |
360 |
100% |
360 |
100% |
The respondents were asked about their involvement in peer group and their responses are as follows: 58.6% of respondents from both the group feel that they are highly involved in peer group and around 40% of the respondents feel that somewhat involvement in peer group. But a few- 1.1% from intervention group and 0.8% from control group feels they have no involvement
|
Component |
Involvement in the Peer group |
Control Group |
Intervention Group |
||||
|
Baseline |
Post- intervention |
Follow- up |
Baseline |
Post- intervention |
Follow- up |
||
|
Somatic Symptom |
Highly involved |
6.981 |
6.901 |
6.872 |
7.033 |
3.308 |
5.815 |
|
Somewhat involved |
7.158 |
7.048 |
6.973 |
7.572 |
3.166 |
6.400 |
|
|
Not involved |
6.000 |
6.000 |
6.000 |
9.000 |
3.250 |
7.500 |
|
|
Anxiety Symptom |
Highly involved |
6.810 |
6.735 |
6.701 |
6.853 |
3.180 |
5.649 |
|
Somewhat involved |
7.575 |
7.438 |
7.404 |
7.793 |
3.476 |
6.510 |
|
|
Not involved |
6.667 |
6.667 |
6.667 |
7.250 |
2.500 |
5.750 |
|
|
Social Dysfunction |
Highly involved |
7.701 |
7.654 |
7.635 |
8.071 |
3.498 |
6.929 |
|
Somewhat involved |
7.904 |
7.829 |
7.801 |
8.310 |
3.310 |
7.110 |
|
|
Not involved |
9.333 |
9.333 |
9.333 |
13.000 |
5.000 |
11.500 |
|
|
Severe Depression |
Highly involved |
7.251 |
7.194 |
7.161 |
7.507 |
4.000 |
6.189 |
|
Somewhat involved |
6.986 |
6.884 |
6.843 |
7.228 |
3.393 |
6.048 |
|
|
Not involved |
10.333 |
10.000 |
10.000 |
12.250 |
4.250 |
10.000 |
|
|
Total Mental Health |
Highly involved |
28.744 |
28.483 |
28.369 |
29.465 |
13.986 |
24.583 |
|
Somewhat involved |
29.623 |
29.199 |
29.021 |
30.903 |
13.345 |
26.069 |
|
|
Not involved |
32.333 |
32.000 |
32.000 |
41.500 |
15.000 |
34.750 |
|
|
Mental Wellbeing |
Highly involved |
43.706 |
43.948 |
44.052 |
45.147 |
55.616 |
47.602 |
|
Somewhat involved |
42.623 |
42.939 |
43.034 |
42.283 |
54.248 |
44.572 |
|
|
Not involved |
43.333 |
43.333 |
43.333 |
37.000 |
55.750 |
40.250 |
|
Table 4Average scores of various components on peer group involvement
The above table shows that the effect of involvement in peer group in different time lines of pre- post and follow-up intervention. The result shows that the involvement in peer group is significant in post- intervention scores in various components of the intervention group. It is observed that somewhat / balanced involvement is better for maintaining good mental health and wellbeing.
This study shows that, life skills training have positive impact on mental health and wellbeing and significantly influenced by the involvement in peer groups. The average score of mental health is in its maximum at the baseline (pre-intervention) level, then reduced to minimum at the post – intervention level but increased again in the follow – up intervention level (lower score represents better mental health status). But in the case of mental wellbeing score, it is reflected that, the average score is in its minimum at the baseline, then increased to maximum at post- intervention but decreased again in the follow-up intervention level (higher score represents better wellbeing).
Considering the involvement of peer group, it is noticed that mental health and wellbeing scores are better for the respondents those having somewhat/balanced involvement with peer groups compared to those who have high involvement or do not have peer group involvement. And also, it can be observed that these scores are better especially in post-intervention level of the intervention group and it emphasizes that young people need constant support and periodic intervention to maintain mental health and wellbeing in day today life. The intervention being proved to be effective, leads to the conclusion that life skills training is effective to enhance mental health and well being and further that somewhat or balanced involvement in peer groups has a significant influence on mental health and wellbeing of young people.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org