
Ashok Garg 1, Deepak Agrawal 2*, Deepika Mishra 3, G L Sharma 4
1 Senior Consultant and Head, Department of Preventive and Non invasive Cardiology, Jaipur Heart Institute, Jaipur
2 DNB Cardiology Consultant Cardiology, Jaipur Heart Institute, Jaipur
3 Pathology Professor, Department of Pathology, SMS Hospital, Jaipur
4 DM Cardiology Consultant Interventional Cardiologist, Jaipur Heart Institute, Jaipur
*Corresponding author: Deepak Agrawal, MBBS, MD (General Medicine), DNB Cardiology Consultant Cardiology, Jaipur Heart Institute, Jaipur
Received: April 25, 2021
Accepted: May 10, 2021
Published: May 19, 2021
Citation: Ashok Garg, Deepak Agrawal, Deepika Mishra, G L Sharma “Autoimmune Disorders: A Brief Appraisal”. Clinical Case Reports and Clinical Study, 3(4); DOI: 10.61148/2766-8614/JCCRCS/063
Copyright: © 2021 Deepak Agrawal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
A 35 years old normotensive, non-diabetic female having 3 children presented with complaints of palpitation and breathlessness from last 2 years, which increased since last 15 days. She did not have any history of fever, cough, chest pain or syncope.
Introduction
A 35 years old normotensive, non-diabetic female having 3 children presented with complaints of palpitation and breathlessness from last 2 years, which increased since last 15 days. She did not have any history of fever, cough, chest pain or syncope.
On examination, her pulse rate was 86/minute regularly regular and her systemic Blood Pressure was 110/50 mm Hg. Her Oxygen saturation was 97% on room air. General physical examination was unremarkable with no clinical features suggestive of Marfan’s syndrome, rheumatic heart disease or infective endocarditis. Cardiovascular examination revealed a long diastolic murmur in left 3rd intercostal space & continuous murmur in left infraclavicular area. Cardiac apex was in left 6th intercostal space lateral to midclavicular line, suggestive of cardiomegaly.
Her ECG revealed downsloping ST segment depression with T wave inversion in leads I, II, III, aVF, aVL & V6 with tall QRS complexes in leads V4-V6, consistent with changes of LV volume overload (Figure 1).
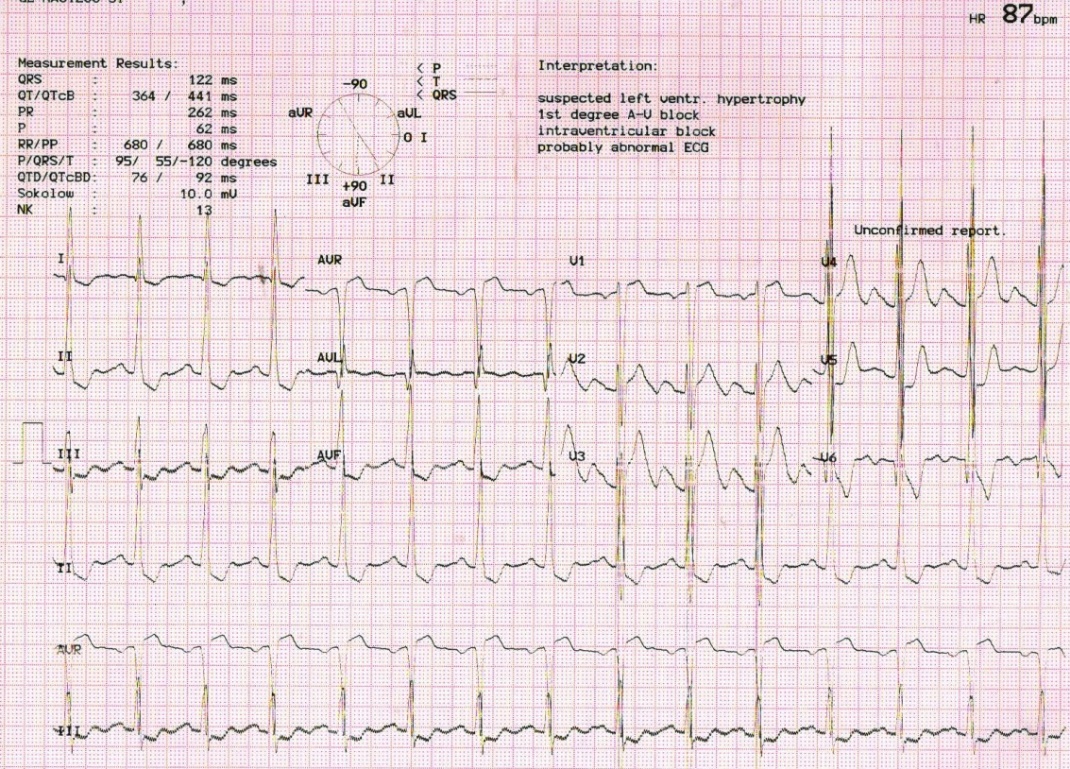
Figure 1: ECG of patient suggestive of LV volume overload.
Her 2D echocardiography revealed dilated left ventricle (LVEdD 66.6 mm) with severe aortic regurgitation (vena contracta size 6.85mm) in association with severe aortic valve stenosis (Peak /Mean gradient across aortic valve = 111.2/73.0 mmHg) (Figure 2 & 3).
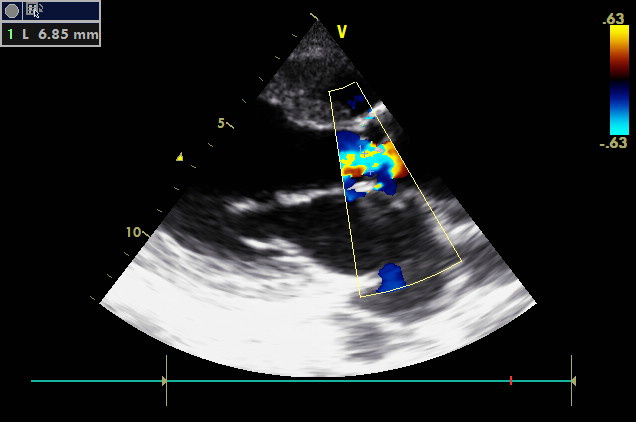
Figure 2: Parasternal long-axis view showing severe aortic regurgitation with vena contracta width of 6.85 mm.
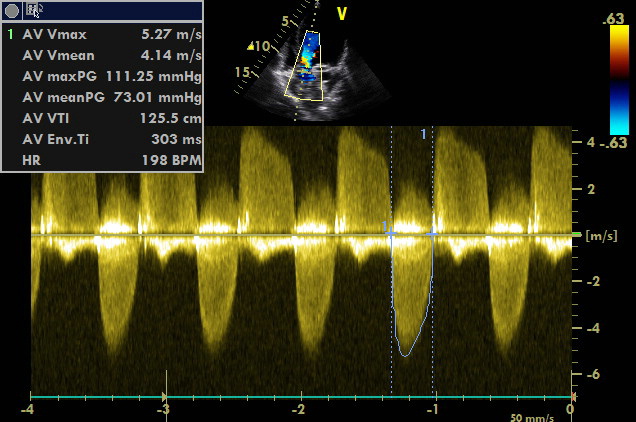
Figure 3: Apical 5 chamber view showing severe aortic stenosis with peak/ mean pressure gradient across valve = 111.25/ 73.01 mmHg.
Aortic valve was tricuspid in appearance (Figure 4).
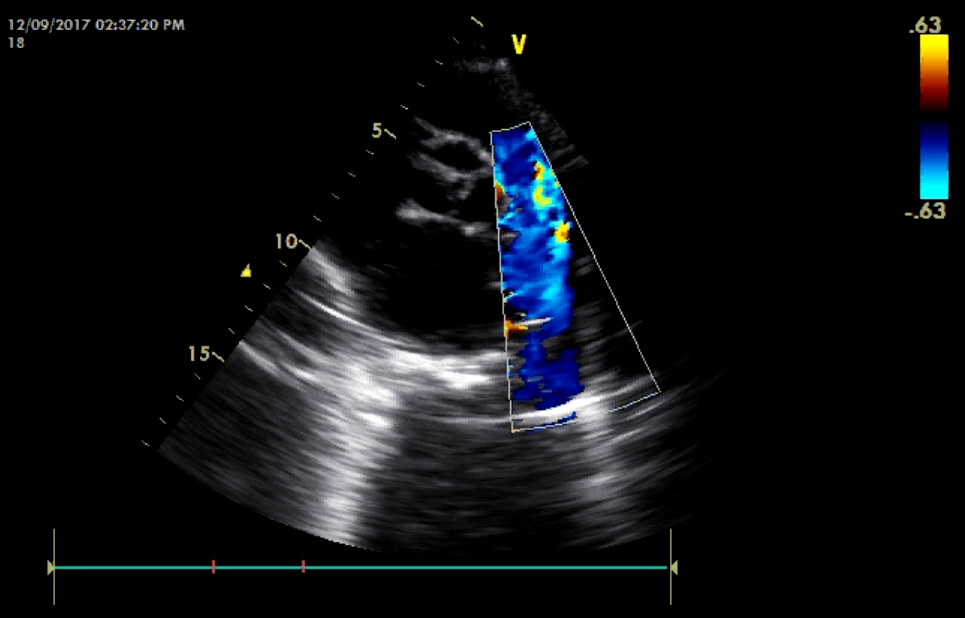
Figure 4: Parasternal short-axis view showing tricuspid aortic valve.
There was no subaortic membrane.
Interestingly, there was also presence of Patent ductus arteriosus (PDA) of size 6.73 mm with left to right shunt. Systolic/ Diastolic gradient across PDA was 83.9/28.1 mmHg (Figure 5 & 6, Video 1).
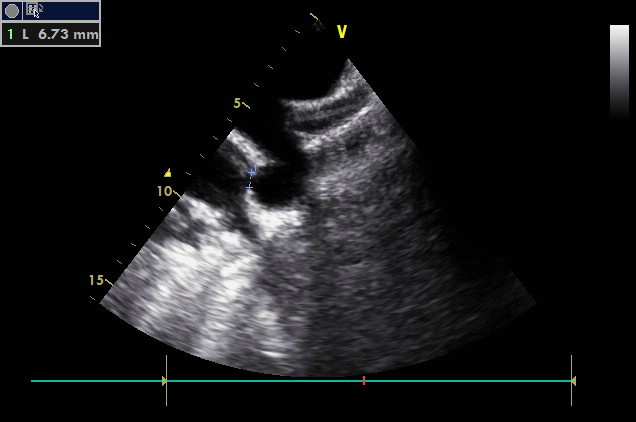
Figure 5: Suprasternal view showing PDA of size 6.73 mm.
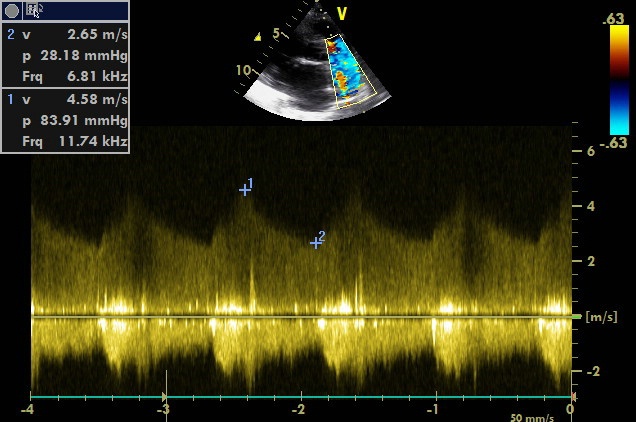
Figure 6: Continuous flow across PDA with peak gradient of 83.91 mmHg
There was mild tricuspid regurgitation (TR) with peak pressure gradient across tricuspid valve was 54.3 mmHg.
Simultaneous occurrence of aortic stenosis and patent ductus arteriosus requiring surgical repair is not unusual in the pediatric population but has rarely been reported in the adult. A rare association of patent ductus arteriosus and bicuspid aortic valve was reported by Ramakrishna et al. Both subvalvular aortic stenosis and bicuspid aortic valve causing aortic stenosis have been reported with patent ductus arteriosus. After extensive search in the literature, we could not find any case of patent ductus arteriosus associated with sever aortic regurgitation.
Our current case is unique in the sense that PDA was associated with severe aortic regurgitation and tricuspid aortic valve with aortic stenosis, which seems to be of rheumatic etiology.
Funding Support: nil
Conflict of interest: nil
,

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org